Routine work with urine microscopy can lead to plenty of “surprises.” Sometimes not only the microscopic evaluation presents something new and unique, but the findings can be observed directly by looking at the sample. The original post on the visible sediment explains very well examples of macroscopic findings.
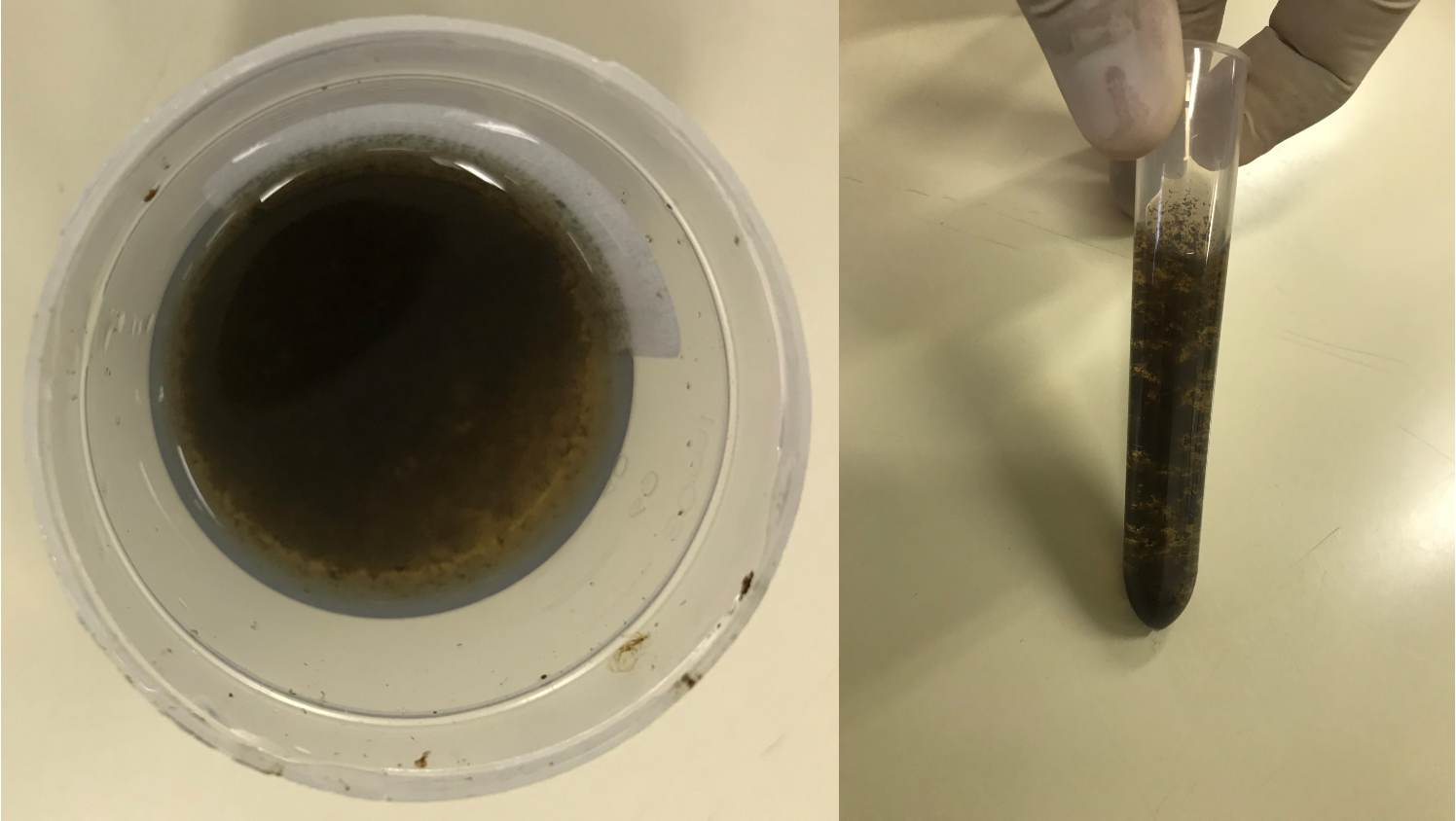
Here we return to the visible sediment to show something that is not a routine finding. To be very honest, at first glance, I thought the patient collected a swamp water sample and sent it to the laboratory (Figure 1).
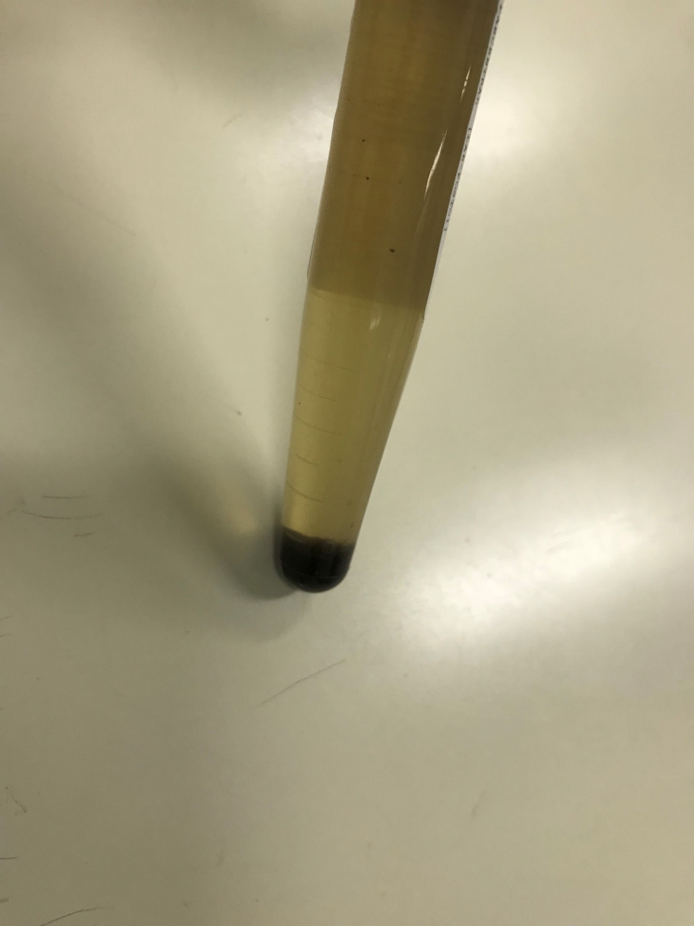
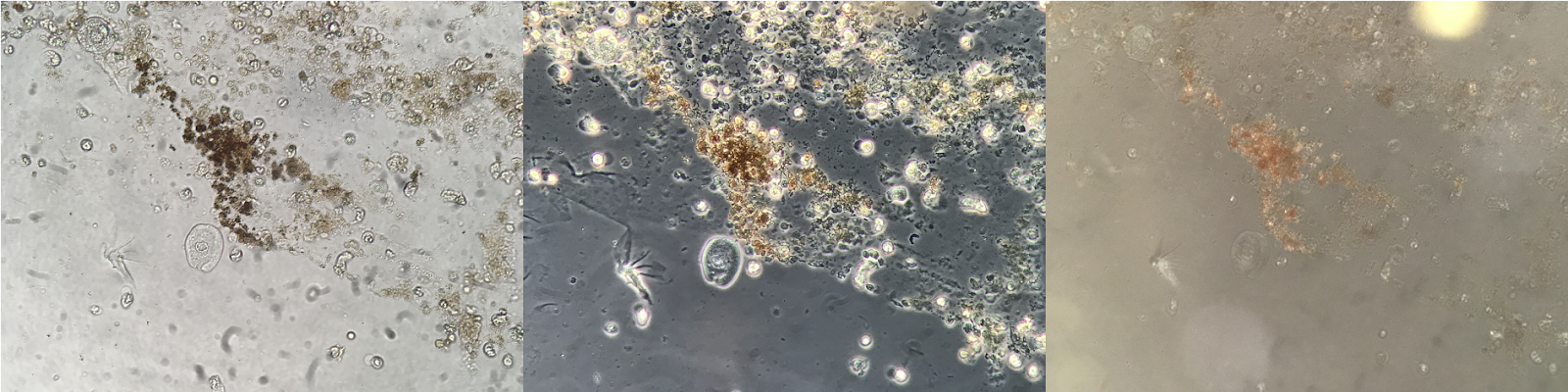
After centrifuging the sample, there was a large amount of sediment in the bottom of the conical tube (Figure 2). At the microscope level, there was a large amount of isomorphic erythrocytes, leukocytes and amorphous material (Figure 3) that did not match with urates or phosphates granules.
The patient’s clinical history was the key to better interpret this urine sample. I learned that the sample was from a 28 year-old male patient who had received a kidney transplant at age 8. His transplant surgery was unique in that he had a procedure called a gastrocystoplasty: a controversial procedure, first described in 1950, that uses gastric tissue in the reconstruction of the lower urinary tract. This procedure is mainly used as an alternative to intestinal cystoplasty (colocystoplasty or ileocystoplasty). The unique advantage is having a “new bladder.” The disadvantages of a gastrocystoplasty include peptic ulcer in the bladder, perforation of the gastric segment, hyponatremic hypochloremic alkalosis, hypergastrinemia, formation of secondary tumors and hematuria-dysuria syndrome.
Given the patient’s presentation and clinical findings, hematuria-dysuria syndrome is possible. This syndrome is characterized by symptoms such as bladder spasms, suprapubic, penis or periurethral pain, coffee brown or macroscopic hematuria without urinary infections; excoriation of the skin, and/or dysuria without infection.
The etiology of hematuria-dysuria syndrome is not completely known. The decrease in the pH of the urine was not a significant association, although other authors have reported a difference between bladder mucosa and urinary pH. Patients with irritative urinary symptoms have responded well to histamine receptors 2-blockers, leaving aciduria as the possible etiology of the syndrome. Some authors have attributed high gastrin levels as a cause of hematuria-dysuria syndrome, although others found no direct relationship between gastrin levels and irritative symptoms. Another possible factor involved in the etiology has been the Helicobacter pylori, which was diagnosed using ELISA technique.
The Important take home message here is the macroscopic evaluation of the urine was helpful to understand and uncover the patient’s clinical history.
Post by: José Antonio Tesser Poloni
Reviewed by: Margaret DeOliveira, Samira Farouk