Erythropoietin stimulating agent (ESA) dosing is a black box of knowledge until you go into nephrology or hematology. Especially between hospitalized patients and dialysis units and outpatient clinics. Maybe this will be obsolete with HIF inhibitors (or we will need new conversion tables), but for now ESAs reign.
There are many ESAs on the market as detailed in the table below. Not listed is epoetin alpha-epbx (Retacrit) by Pfizer, which is a “biosimilar.” It’s a fancy word that means Retacrit is essentially the same in terms of safety and efficacy to Procrit, so it can sometimes get approved faster and is cheaper. All the epoetin alfa products can be interchanged at the pharmacy level, but to convert to and from Retacrit, you need a new prescription.
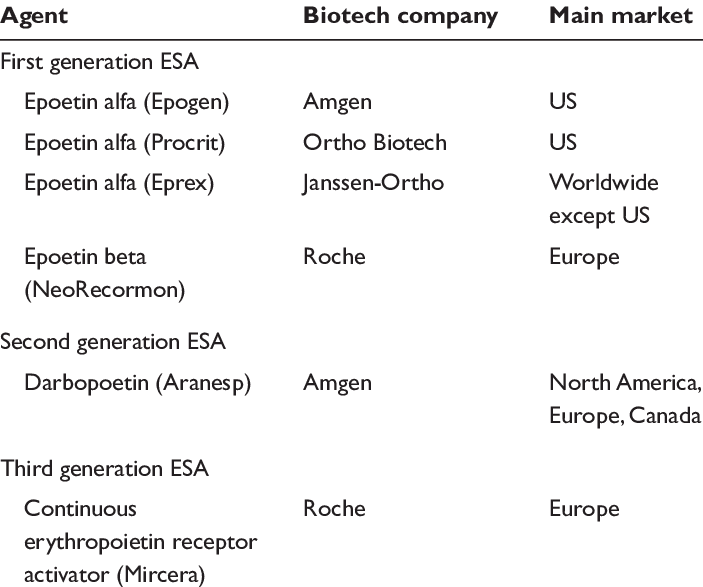
All forms of ESAs are approved for anemia in CKD and dialysis patients in adults. Only darbepoietin and methoxy polyethylene glycol-epoetin beta (MiceraⓇ) are approved for children on dialysis. Darbepoietin can be dosed weekly, every 2 weeks, or every 4 weeks. MiceraⓇ is dosed every 2-4 weeks.
Because I am based in the US, I am only familiar with the conversion between US dosing.
| IV | SQ | |
| epoetin | 2 | 1 |
| darbepoetin | 1 | 1 |
| methoxy polyethylene glycol-epoetin beta | 1 | 1 |
The subcutaneous (SQ) dosing of epogen is roughly half that of the IV dose, likely due to its longer half-life when given SQ.
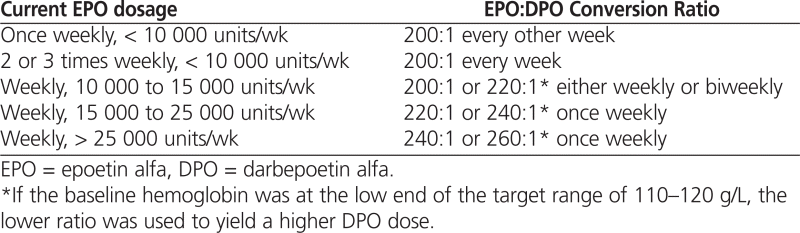
When converting IV epoetin to IV darbepoetin, the manufacturer recommends a 200:1 dosing (ie 200 units of epoetin to 1 unit of darbepoetin). But in real life depending, this ratio may likely over-treat your patient. Different studies have found ratios anywhere from 275:1 or 300:1 to 350:1. The higher your weekly epoetin dose, likely the higher the conversion ratio.
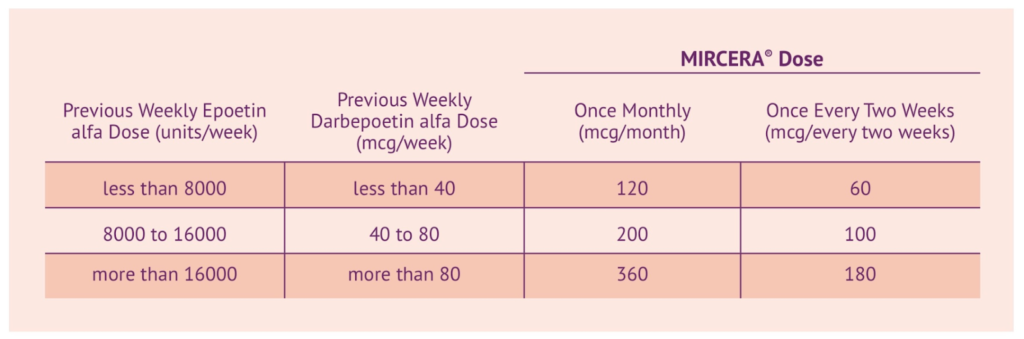
Conversion to methoxy polyethylene glycol-epoetin beta (MiceraⓇ) is a little tricker. The manufacturer has a nice conversion table they publish, but essentially the MiceraⓇ dose every 2 weeks is roughly 1.5 times the darbepoetin weekly dose.
Hope this helps!

