Sriram Sriperumbuduri MD DM DRCPSC
Nephrology Fellow
The Ottawa Hospital, Ottawa Canada
@sriperumbuduris
Catheter dysfunction in peritoneal dialysis (PD) is a common complication leading to diminished quality of life, reduced dialysis and the potential to abandon PD and transition to hemodialysis (HD). While a majority of PD catheter dysfunctions can be managed with simple strategies, like the treatment of constipation, some cases involve dealing with multiple pathophysiologic mechanisms in the same patient and thus require more than one intervention.
Definition and prevalence: There is no universally accepted definition of PD catheter dysfunction. Different statements were provided by various authors including-
- “Normal or reduced inflow accompanied with slow drainage or no drainage of infused dialysate”“poor drainage or poor inflow or associated pain, or any combination of these, and no evidence of pericatheter leakage”.
- Simplified definition- a problem with inflow or outflow or both, should be considered PD catheter dysfunction.
Prevalence rates vary depending on the center, experience of the surgeon, and the definition adopted. In one study from Fisher et al (1985), prevalence was 20%, whereas others quoted rates varying between 4%– 13%.
Signs and symptoms: PD catheter dysfunction presents differently based on the modality of PD being used. Patients on continuous cyclic peritoneal dialysis- CCPD (cycler) typically present with low drain alarms. While those on continuous ambulatory PD (CAPD) have prolonged fill or drain times. Alarms have a significant impact on sleep and thus, the quality of life in both the patients and their partners. In some cases, we may find increased lost dwell times (discussed in detail below) recorded in the daily PD sheets of asymptomatic patients.
What is lost dwell time? Before going into the details of the topic, we will look at what is lost dwell time and when and why it is significant?
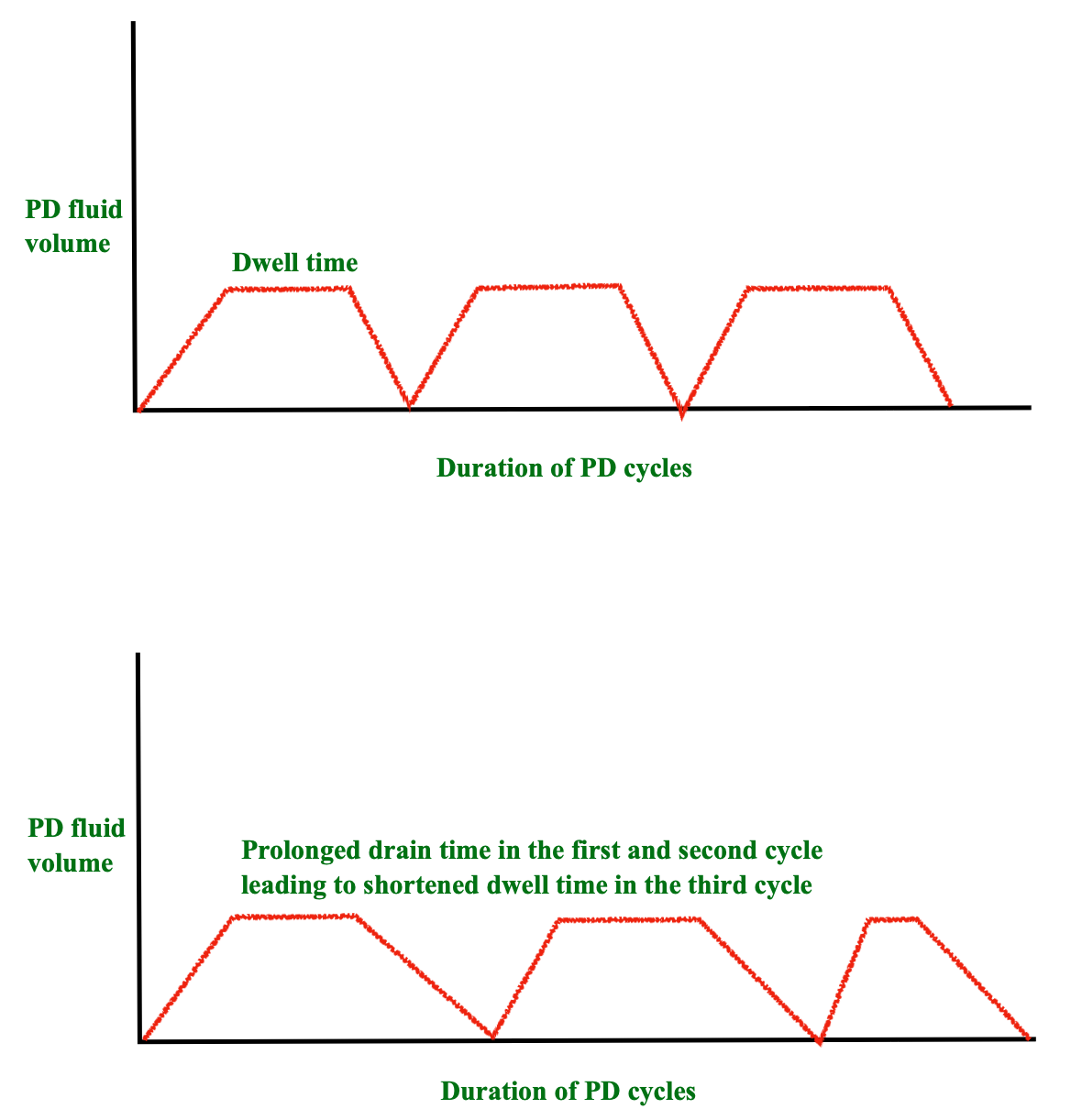
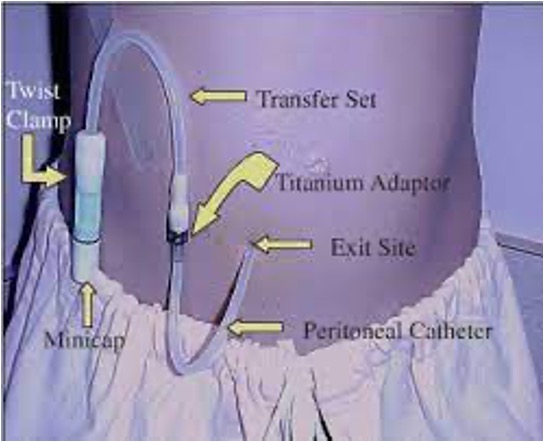
Each cycle during PD (Figure 1) consists of inflow of the fluid, followed by dwell time when dialysate is contacting the membrane and dialysis is occurring and outflow/ drainage of the fluid. The dwell time is critical, as the process of dialysis (diffusion) happens during this phase. The standard PD cycler settings include a smart program which will vary dwell time in response to fill/drain time to maintain the total therapy time as prescribed. Thus, a patient will receive 8 hours of dialysis a night if prescribed, but may not receive the fully prescribed dwell time if catheter dysfunction is present. If there is a problem with inflow or outflow, the machine will spend more time filling or draining the patient and less time during the dwell phase. This leads to loss of dwell time on the cycler, and thus loss of effective dialysis time.
There is no universally accepted definition for significant lost dwell times. However, a commonly used metric is lost dwell time that exceeds 30 minutes during a night on the cycler. Usually if the patient is losing dwell times >30 minutes for 2 or more nights in a week, we evaluate the patient for possible PD catheter dysfunction.
Causes of PD catheter dysfunction
This can be categorised into 2 groups:
- Patient-related eg. constipation
- Catheter-related eg. migration of catheter tip, omental wrap, adhesions, etc.
Others have categorized the etiology into two groups- one way- or two way- catheter obstruction, as in this previous post.
Patient-related cause(s)
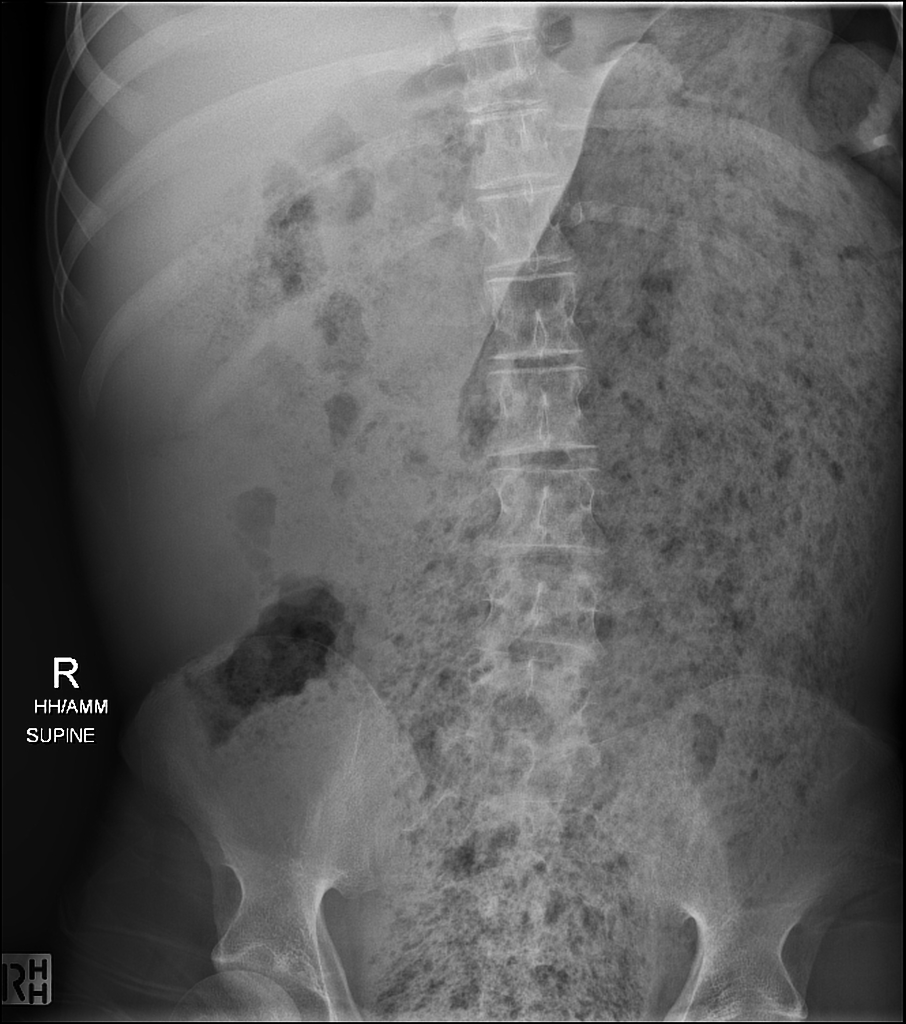
The most frequently encountered patient-related cause of increased lost dwell time is constipation. This is shown in the abdominal x-ray (AXR) below in Figure 2.
A literature review described 5 research studies pertaining to constipation in this population. The salient features of this paper include-
- Major factors contributing to constipation are restriction of diet and fluid, use of phosphate binders and potassium binding resins.
- Studies by Yasuda et al and Sutton et al showed that increased use of dietary fibre (fruits and vegetables) was effective in decreasing the incidence of constipation.
- Most of the above studies described constipation from a patient’s perspective. This limited the specificity and sensitivity of these studies.
- Use of standardized definitions like Rome 4 criteria for constipation and Bristol stool form scale are helpful in estimating the true prevalence of constipation. Patients should be made aware of these criteria during their training, to help them accurately identify constipation.
- A prospective study by Mimidis et al showed the benefit of polyethylene glycol (PEG) in a dose of 17 gm (in 250 ml solution) given as 2 divided doses daily for 8 weeks in improving bowel movements, including frequency, consistency along with decrease in painful defecation and rectal irritation. The study was done in 25 patients, of which 21 completed the protocol and had benefit with the drug.
Management of constipation involves use of laxatives including senokot, lactulose and PEG, among others. Frequently, empiric treatment of constipation is undertaken as a first step in management of catheter dysfunction. Use of phosphate– and magnesium– containing cathartic agents in patients with kidney dysfunction is associated with risk of acute kidney injury and hypermagnesemia respectively and should be avoided.
Catheter-related causes
Frequently encountered causes include-
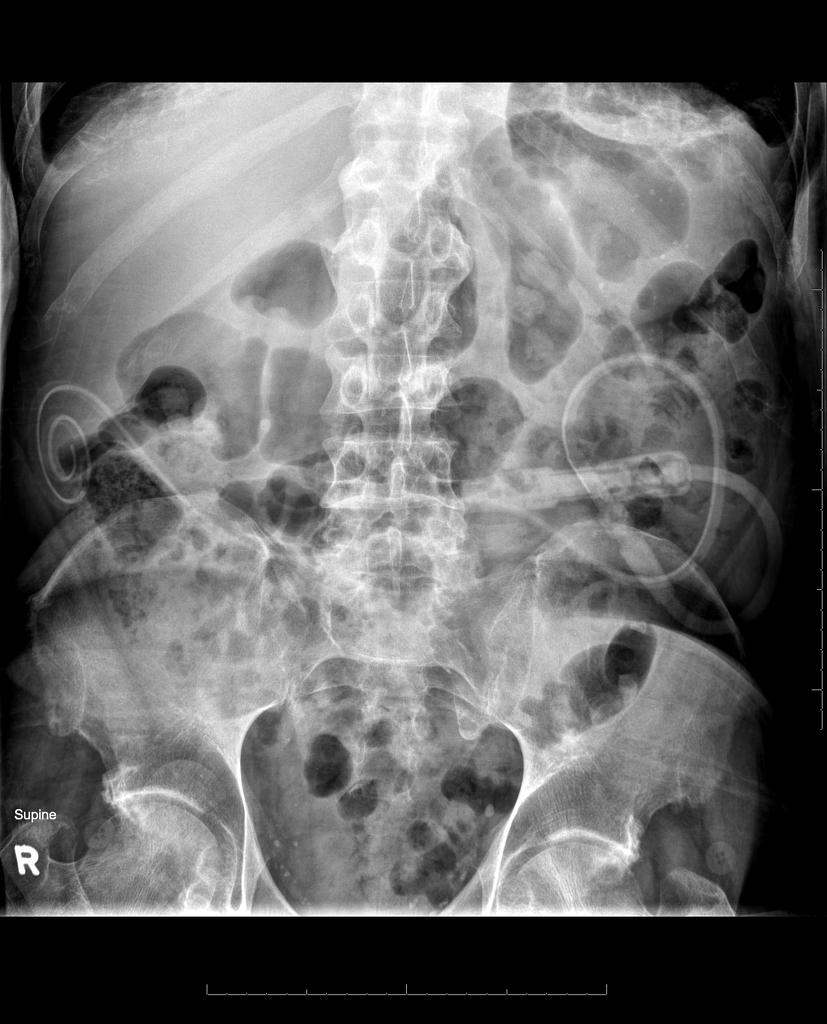
Catheter tip migration seen in Figure 3
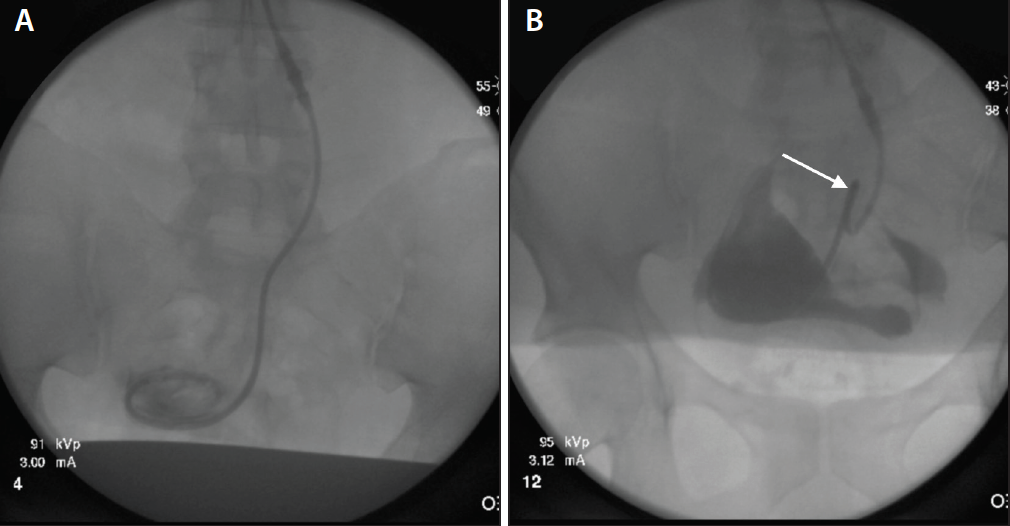
Omental wrap and Omental/ bowel adhesions Distinguishing isolated tip migration from migration with omental wrap or adhesions requires fluoroscopic imaging and radiocontrast injection into the PD catheter. If there is no significant pericatheter stasis of contrast, this represents catheter tip migration. In cases of complex filling defects at the tip or stasis of contrast around the catheter, suspect extraluminal obstruction eg. omental wrapping or adhesions.
Catheter kinking: internal or external portion of the catheter. Diagnosis of kink in the internal portion of the catheter frequently requires imaging with at least two views -Anteroposterior (AP) and lateral. Very short portion of the external part of the catheter could predispose to kinking at the level of the adapter (Figure 5).
Malposition of Cycler:
- Presence of a cycler on the side opposite to the PD catheter exit site could potentially stretch the catheter and cause kinking.
- Placing the cycler at a level that is higher or lower than the level of the patient.
A study from The Ottawa hospital showed that the presence of buried PD catheters for >4.4 months increases the risk of catheter dysfunction due to fibrin plugging, tip migration and omental entrapment.
Catheter dysfunction frequently requires fluoroscopic or laparoscopic manipulation of the PD catheter for diagnosis and treatment. A retrospective study by Miller et al looked at the outcomes and factors associated with fluoroscopic manipulation of PD catheters. A set of interventions were done prior to labelling the catheter obstruction as refractory. The interventions included were shown in the table 1 below.
| Poor Inflow | Poor Outflow |
| Vigorous push and pull technique- 30 ml syringe for 5 minutes | Flushing with heparinized saline |
| tPA (1 mg/ ml) 7 mg instilled, followed by 1 mg every 15 minutes for another 3 mg and left overnight | use of high-dose laxatives |
| Repeat attempt to flush the next day | AXR |
| Fluoroscopic manipulation | Fluoroscopic manipulation |
During the fluoroscopic manipulation, the guidewire was used to clear any fibrin and straighten the coiled tip of the catheter, thus freeing the catheter from any fibrin sheath or adhesions. Primary outcome in the study was successful manipulation which was defined as adequate catheter function to permit PD at 30 days.
The success rate of fluoroscopic manipulation was about 60%. The two factors associated with the successful outcome included the presence of catheter tip in the true pelvis and secondary failure of PD. Secondary failure is defined as inability to do PD after some period of functioning as opposed to primary failure when the catheter never worked after exteriorization.
One study from Taiwan described the salvage of malfunctioning PD catheters in 11 patients with a minilaparotomy approach to free the adhesions and resumption of PD on the same day. Another study from Turkey described a laparoscopic approach for the management of PD catheter dysfunction in 40 patients and PD was resumed with low volumes on the first post operative day.
Role of fibrin clots in PD catheter dysfunction: Another frequent cause of poor catheter inflow and outflow is the presence of fibrin clots (Figure 6) in the PD catheter lumen. This is well documented in literature as in a recent case series from Australia.
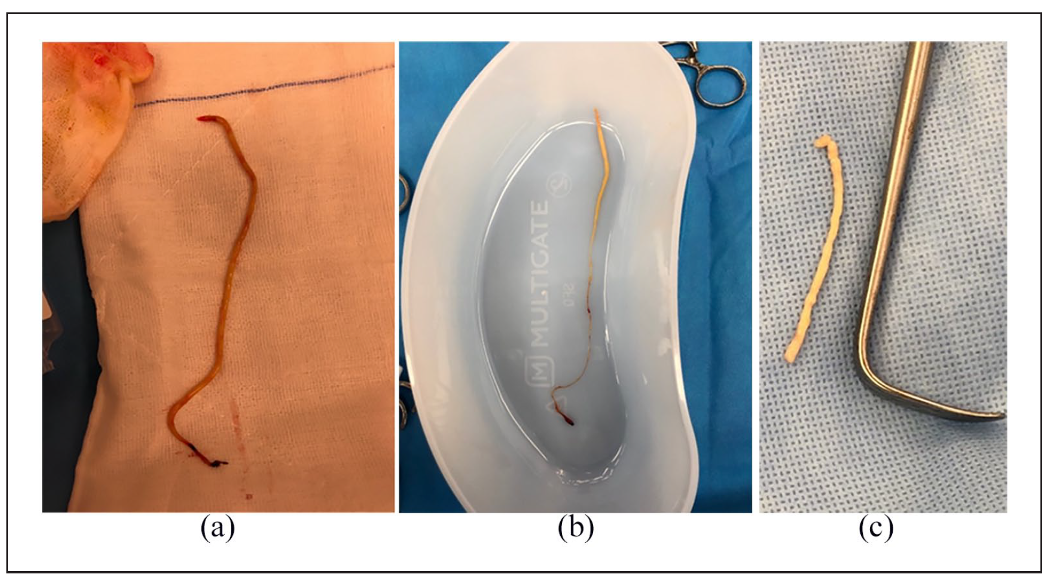
All the 3 cases described in this study involved surgically placed buried PD catheters and required surgical revision to remove the clots. The role of tissue plasminogen activator (tPA- Alteplase) was well described in literature in the management of fibrin clots. This was more commonly reported in the pediatric population, due to higher risk of catheter occlusion attributed to smaller size of the catheter lumen. The dose of tPA varies between 1-10 mg with dwell times of 1-2 hours depending on the hospital protocol.
Complete occlusion of the PD catheter will decrease the surface of the clot that can be lysed by tPA, thus commonly requiring surgical manipulation to dislodge the clot. Previous case series described the use of an endoscopic cleaning brush (Channel cleaning brush, OlympusBW-20T) to clear the contents under fluoroscopic guidance.
Other uncommon causes of catheter obstruction were documented in literature including encasement of the internal portion of the catheter in an encapsulating sheath. Two interesting hypotheses were proposed behind the formation of this dense and encapsulating covering with evidence of vascularization -1. Reaction to normal saline (See this intriguing article by Oreopoulus) 2. Small, but clinically significant bio-incompatibility of silicone catheter.
Membrane-related causes
Although this cannot be categorized as a cause of catheter dysfunction, certain peritoneal membrane characteristics can potentially lead to prolonged lost dwell time and may mimic true catheter related malfunction. This may be seen in the presence of high transporter status.
Peritoneal equilibration test (PET) in a patient with high transporter/ high average status has the following characteristics (Figure 7).
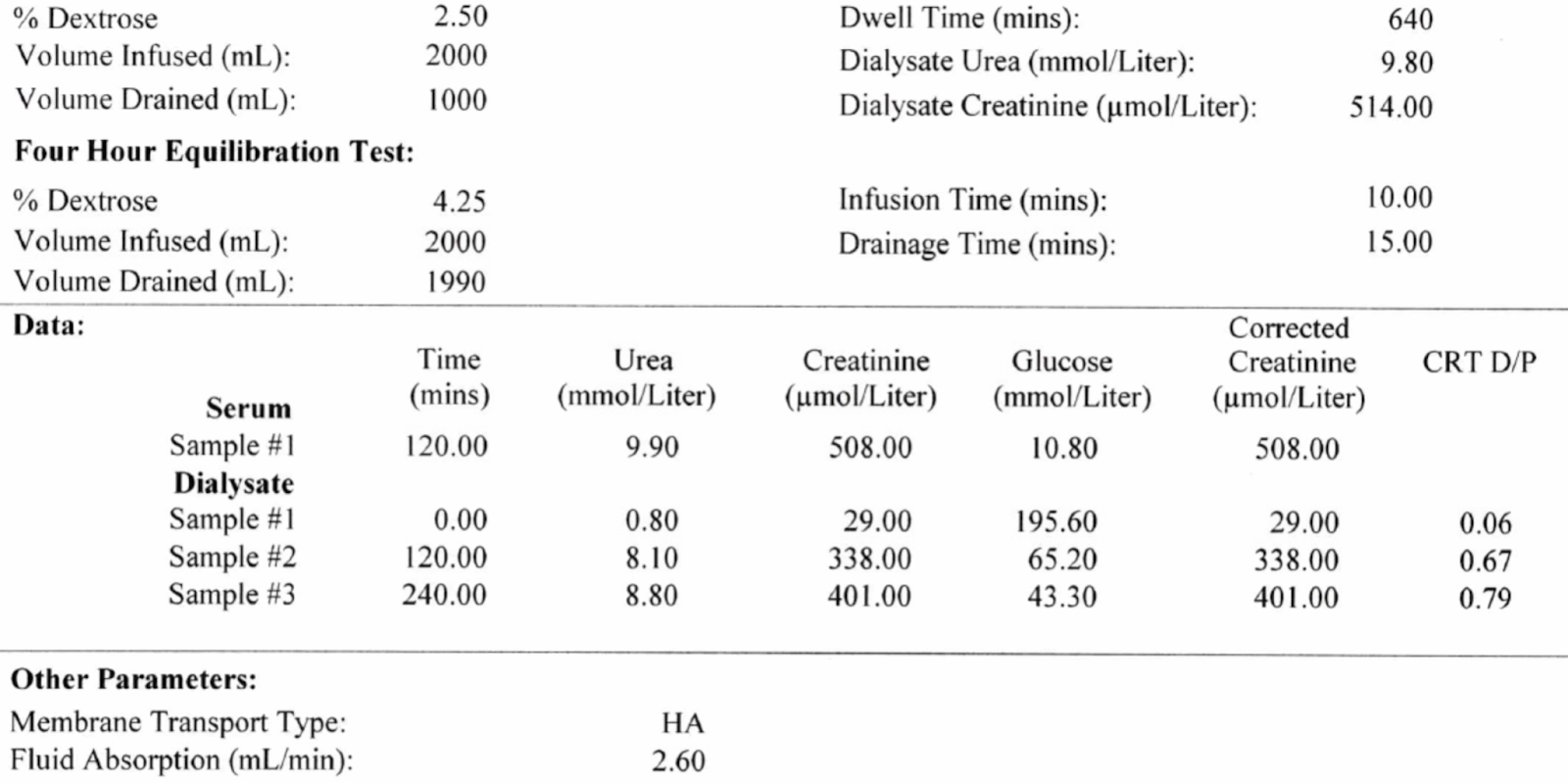
As shown in the figure, high transporter status is associated with increased absorption of fluid from the dialysate leading to decreased and sometimes negative ultrafiltration. Use of shorter dwell times will prevent fluid absorption and avoid losing excess dwell times.
In the next part, I will discuss the role of tidal PD and give a brief overview of steps involved in management of patients with PD catheter dysfunction
Reviewed by Matthew A. Sparks
Great content! This is exactly the sort of thing I was looking for. Thanks for your help
very nice and useful post.
I am interested to know how much percentage of catheter malfunction will be managed conservatively I mean with flushing and treatment of constipation or by tPA VS need for laparoscopic intervention or fluoroscopic guided manipulation in your center if any data is there?