The rate of patients >75 years of age initiating dialysis has grown substantially in the U.S. over the past two decades. This has to do with several factors, including improvements in medical technology enabling people to live long enough to develop advanced CKD, but also an increasing expectation for aggressive medical care late in life. In the U.S., the fact that the Social Security Act in 1972 pays for dialysis in all individuals also plays a role in this statistic. The “Precious Bodily Fluids” blog recently posted an extensive review of the subject in power point presentation form.
But how do elderly patients do once they have started dialysis? The answer is complex–and not surprisingly it depends on the patient. According to several studies, age itself is not a preclusion for starting dialysis–some patients > 90 years old can even do well provided their functional status is reasonable going in. It turns out that the degree of comorbidity a patient has is a much better predictor of how they will do on dialysis than age alone.
As an example, in this 2007 NDT study by Murtagh et al, the investigators performed a retrospective analysis of 129 patients > 75 years of age who were referred to a multi-disciplinary pre-dialysis care clinic. They compared patients who chose dialysis with those who chose “conservative care”–which involved the decision to NOT begin dialysis but rather attempting to control their symptoms with blood pressure control, diet, etc. The primary outcome measured was survival after reaching a GFR of
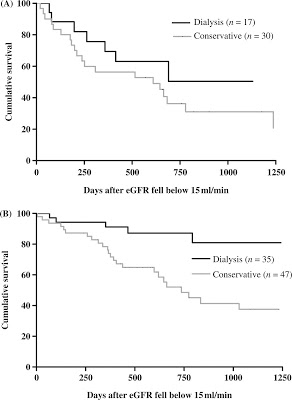
The top graph (A) shows the Kaplan-Meier curve describing patients WITH ISCHEMIC HEART DISEASE as a comorbidity. You can see that the survival advantage in the dialysis group compared to the conservative care group virtually disappears. In the bottom graph (B) is charted patients WITHOUT ischemic heart disease–and shows a robust and obvious survival advantage in the dialysis group.
These factors should ideally be discussed in educating elderly patients about the advantages and disadvantages of starting dialysis. Patients >75 years of age with Stage V CKD and underlying ischemic heart disease should know that their likelihood of dying with or without dialysis is virtually the same. Obviously, every patient is different and deserves to make their own decisions about end-of-life care. But perhaps we should be adopting an evidence-based model similar to what some (not all) oncologists use–in which patients who do not meet a certain performance status are often not even deemed suitable to receive aggressive chemotherapy, with the knowledge that it has the potential to do more harm than good.
Check the full version of the article below. It might help guide your response when patients' relatives ask you… 'how long does my dad/ mom have if he/ she stops dialysis?'
Journal of the American Geriatrics Society
Volume 59, Issue 2, pages 304–308, February 2011
End-Stage Renal Disease: A New Trajectory of Functional Decline in the Last Year of Life
Fliss E.M. Murtagh PhD, Julia M. Addington-Hall PhD, Irene J. Higginson PhD
Article first published online: 28 JAN 2011
OBJECTIVES: To determine the functional trajectory in the last year of life in end-stage renal disease managed without dialysis.
DESIGN: Longitudinal cohort study of functional status over time and toward death.
SETTING: Three renal units in the United Kingdom.
PARTICIPANTS: Patients with Stage 5 chronic kidney disease managed conservatively (without dialysis).
MEASUREMENTS: The main outcome measure was functional status, measured using the Karnofsky Performance Scale.
RESULTS: Seventy-five participants (mean age 80.7, 62% response rate) recruited and followed up monthly for up to 2 years (median 8-month follow-up, range 1–23 months). Forty-nine (66%) died during follow-up. Those who died had similar distribution of age, ethnicity, primary renal pathology, and comorbidity as those still alive at study end. Analysis according to time before death revealed that functional status remained stable during the last year of life but declined steeply in the last month of life.
CONCLUSION: This distinctive renal trajectory, reported here for the first time, contrasts with that previously described in other conditions. This has important clinical implications—the steep functional decline indicates that healthcare services need to be rapidly responsive to changing needs in this population as function declines in the last months and weeks of life
EDGAR LERMA
Chicago
Nice post, and good find from NDT. I will add it to my talk on geriatric kidney disease before I do it again.