I will share with you some of the tips I learned from my pathologist friend Ibrahim Batal.
When evaluating an allograft kidney biopsy for acute changes, you should:First, scan at low power magnification, look for arteries, check for necrosis or infiltration: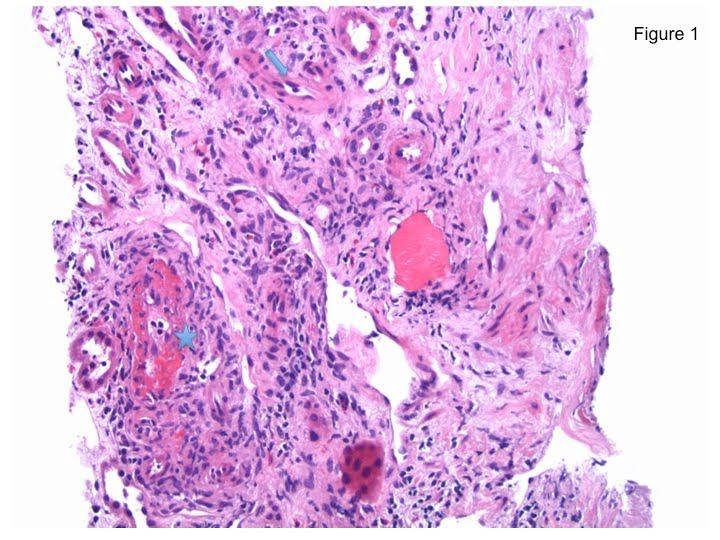 *Fibrinoid necrosis (seen as the red pink color, Figure 1, star) will automatically indicate Banff type 3 T cell mediated rejection TCMR or severe rejection. Compare the Fibrinoid necrosis of this arteriole to the normal arterial tissue seen in Figure 1 marked by the arrow. To review Banff classification review Nate’s prior post.
*Fibrinoid necrosis (seen as the red pink color, Figure 1, star) will automatically indicate Banff type 3 T cell mediated rejection TCMR or severe rejection. Compare the Fibrinoid necrosis of this arteriole to the normal arterial tissue seen in Figure 1 marked by the arrow. To review Banff classification review Nate’s prior post.
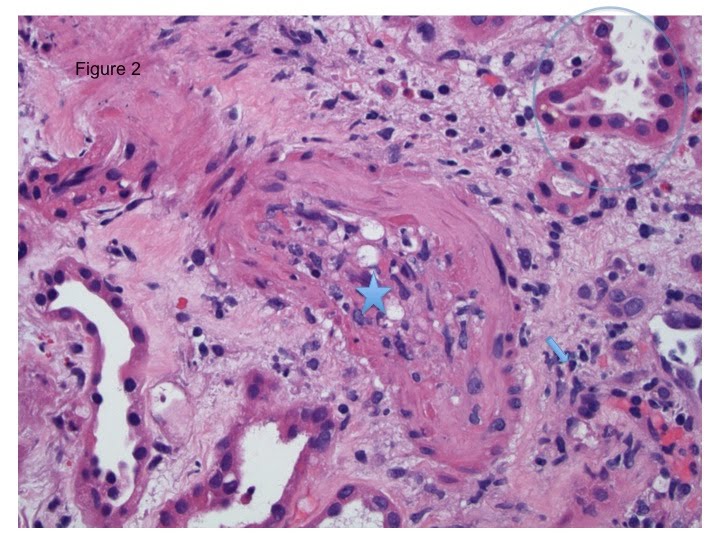 *Infiltrates seen inside the intima of the arteries (Figure 2, star) are lymphocytes and macrophages, which indicate Banff type 2 TCMR. See how the nuclei of those infiltrates look similar to the nuclei of the infiltrates in the interstitium (Figure 2, arrow) but they look different from the tubular epithelial nuclei that are perfectly rounded (Figure 2, circle).
*Infiltrates seen inside the intima of the arteries (Figure 2, star) are lymphocytes and macrophages, which indicate Banff type 2 TCMR. See how the nuclei of those infiltrates look similar to the nuclei of the infiltrates in the interstitium (Figure 2, arrow) but they look different from the tubular epithelial nuclei that are perfectly rounded (Figure 2, circle).
Second, look at the interstitial infiltrates.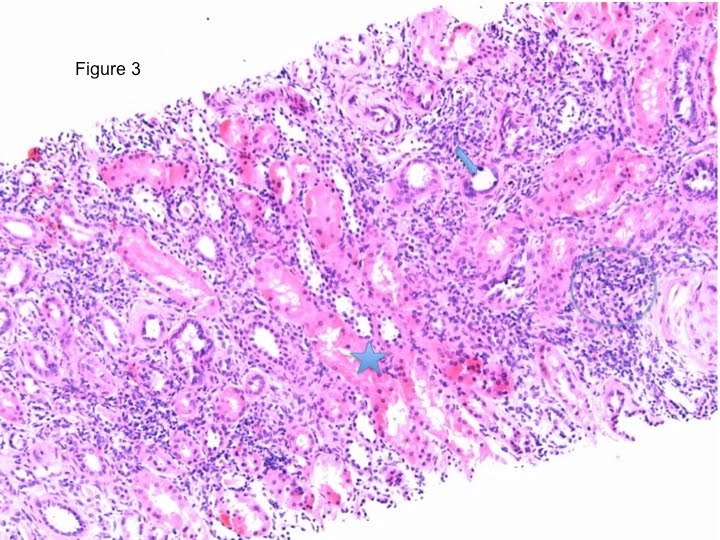 *Normally, the tubules should be packed and back-to-back, if infiltrates exist (Figure 3, blue small cells in the circle), we should be looking at the severity of the tubulitis in the most affected tubule. As you all know the more actively functional proximal tubule has a large strong eosinophilic cytoplasm (Figure 3, star) that differentiate it from the less active small cytoplasm of the distal tubules (Figure 3, arrow).
*Normally, the tubules should be packed and back-to-back, if infiltrates exist (Figure 3, blue small cells in the circle), we should be looking at the severity of the tubulitis in the most affected tubule. As you all know the more actively functional proximal tubule has a large strong eosinophilic cytoplasm (Figure 3, star) that differentiate it from the less active small cytoplasm of the distal tubules (Figure 3, arrow).
To differentiate between the tubular infiltrates and the tubular epithelium itself, compare those cells to the interstitial infiltrates, they should look similar. In addition the leukocytes in the tubules appears darker, sometimes with a hallow surrounding.
Now back to the most affected tubule (Figure 4, circle).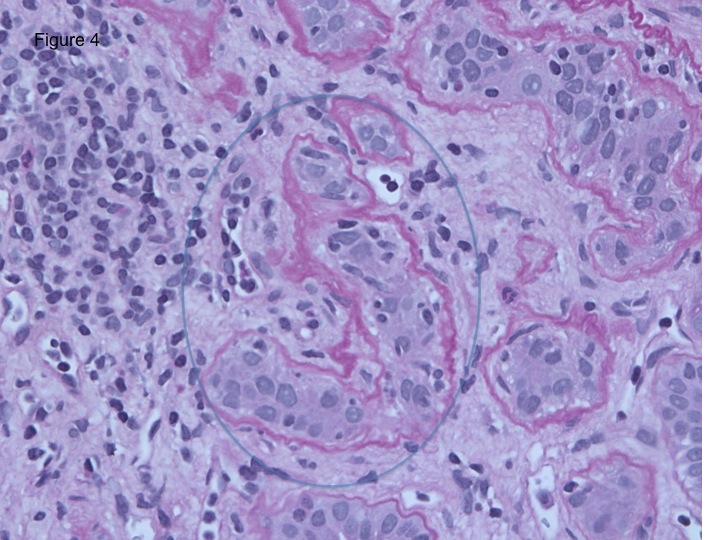
*If the infiltrating leukocytes are more than 10 in the absence of arteriolar infiltrate or necrosis, the TCMR is considered Banff 1B.
*If the infiltrates are between 5 and 10, the TCMR is considered Banff 1A,
*If the infiltrates are 4 or less, the TCMR is considered borderline cellular rejection.
*So imagine the sampling error in this classification.
Now will shift to the acute antibody mediated rejection where the tissue injury is mainly manifested in the microcirculation mainly peritubular capillaries and or glomerular capillaries in its typical form.
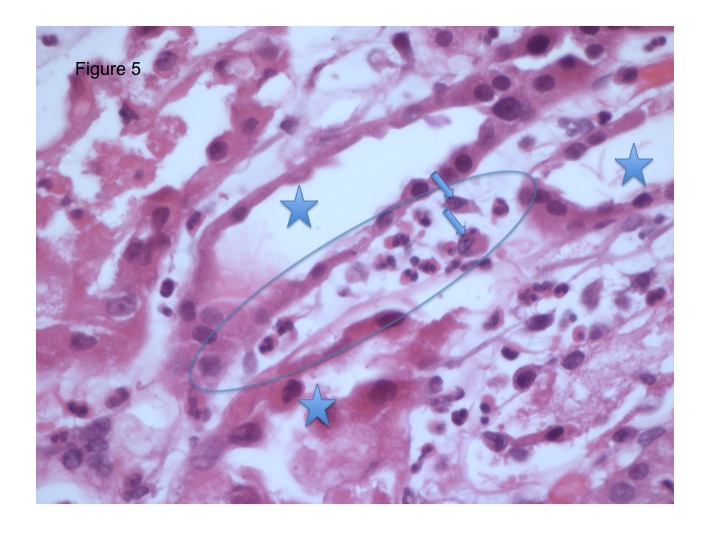 *First, We look at the peritubular capilarities, you have to “imagine” a capillary (Figure 5, circled) between the different surrounding tubules (Figure 5 stars). The “imaginary capillary” is infiltrated by neutrophils (appreciate the multilobular appearance of the nuclei) and macrophages (Figure 5 arrows).
*First, We look at the peritubular capilarities, you have to “imagine” a capillary (Figure 5, circled) between the different surrounding tubules (Figure 5 stars). The “imaginary capillary” is infiltrated by neutrophils (appreciate the multilobular appearance of the nuclei) and macrophages (Figure 5 arrows).
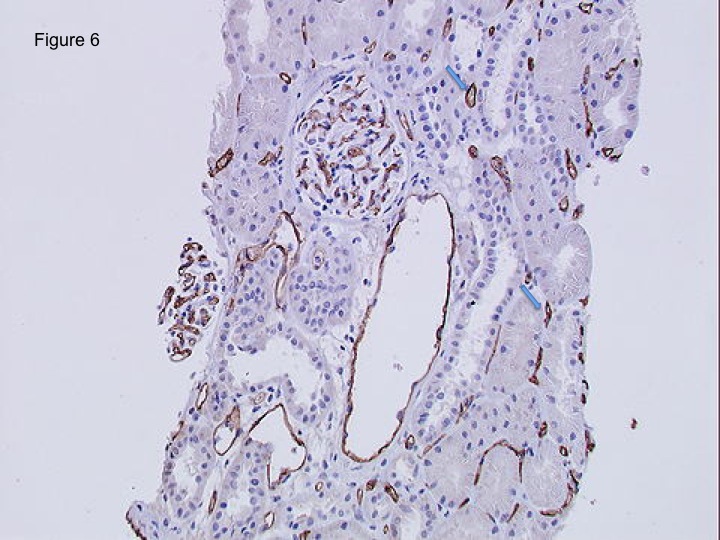 *Second, Because those pathologic manifestations are not sensitive, we always stain for C4d either by immunofluorescence or immunoperoxidase according to the institutions preference, Immunoperoxidase being less sensitive but easier to perform. C4d should be evaluated in the peritubular capillaries (Figure 6, arrow).
*Second, Because those pathologic manifestations are not sensitive, we always stain for C4d either by immunofluorescence or immunoperoxidase according to the institutions preference, Immunoperoxidase being less sensitive but easier to perform. C4d should be evaluated in the peritubular capillaries (Figure 6, arrow).
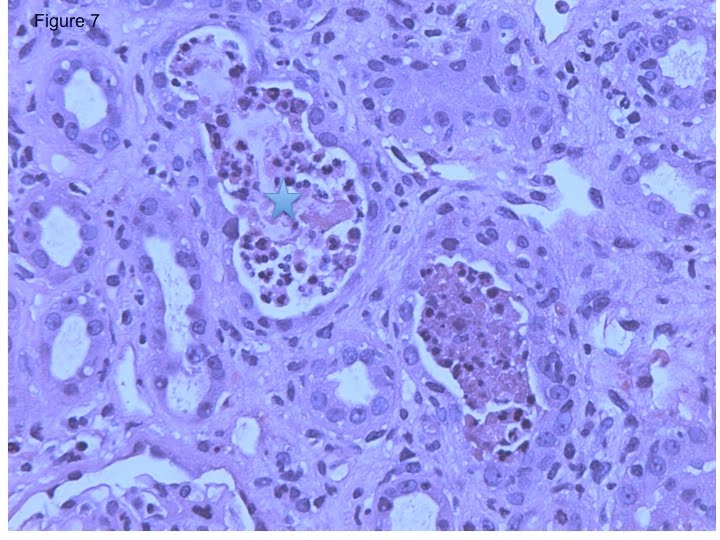 *In contrast to antibody-mediated rejection, when neutrophils are mainly concentrated within the tubular lumen rather than peritubular capillaries (Figure 7, star), then bacterial urinary infection should be high on our differential.
*In contrast to antibody-mediated rejection, when neutrophils are mainly concentrated within the tubular lumen rather than peritubular capillaries (Figure 7, star), then bacterial urinary infection should be high on our differential.
Conclusion: It is always good to have a pathologist as a friend. However, this review should be helpful in trying to interpret renal pathology.

nice one!
it was amazing..hope u will come up with new topics to help DM nephro residents like me
Dr.Manu
it was reaally amazing good picture hope u will help dm residents like us with more topics like this
will try to post some native kidney pathology very soon.Thank you for your interest.
thanksssssssssssssssssssssssssssssss
a lot for your educational hint pls if u can do the same for native kidney biopsy with its variant i will be thanksssssssssssss for u
Thank you for your feedback
Thanks for the positive comments.
great post! keep up the great work!
An excellent educational post! Am posting a link to this on my website