
A glomerular nodule, i.e. an acellular hyaline structure, can have varied etiologies. Most commonly we see it in the setting of diabetic nephropathy (DN). In these cases, it posesses all the associated features of DN on light microscopy (LM) with glomerular basement membrane (GBM) thickening, mesangial matrix expansion and arteriolar hyalinosis. These nodules stain well with PAS & silver stains. Immunofluorescence (IF) shows linear IgG deposits along the GBM & tubular basement membrane (TBM) and occasional IgM & C3 trapped in the sclerotic areas. Electron microscopy (EM) shows similar features.
A differential diagnosis is amyloidosis, associated with enlarged glomeruli but poor staining with PAS and silver stain. The striking feature of this condition is red appearance of nodules on Congo staining with characteristic apple green birefringence under the fluorescent microscopy. In the most common form of amyloidosis, the AL type, IF shows light chain restriction with lambda > kappa predominating. EM has the characteristic amyloid fibrils, 7-12 nm in diameter with indefinite length and random orientation.
Among immune mediated glomerulonephritis (GN), MPGN also presents with nodules on biopsy. LM is highlighted by a proliferative morphology with splitting and duplication of the GBM. Cryoglobulinemic GN is associated with pseudo-thrombi in capillaries, which in fact represent large sub-endothelial deposits. IF shows IgG and C3 deposits in GBM. Cryoglobulinemia is associated with IgM and predominance of kappa deposits (Type 1). EM reveals electron dense deposits in sub endothelial, mesangial and sometimes in sub-epithelial locations.
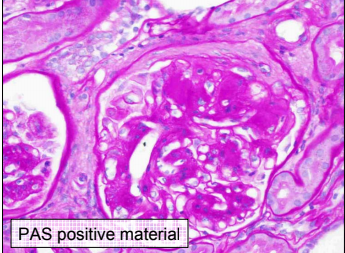 Monoclonal immunoglobulin deposition disease (MIDD) can shows nodules. They stain with PAS and silver stains (see image) and have refractile, PAS-positive deposits in the TBM too. IF is characterized by linear deposits along GBM & TBM with kappa>lambda deposits in LCDD (light chain variant) and IgG in HCDD (heavy chain). EM shows powdery deposits in inner GBM, outer TBM and in the nodules.
Monoclonal immunoglobulin deposition disease (MIDD) can shows nodules. They stain with PAS and silver stains (see image) and have refractile, PAS-positive deposits in the TBM too. IF is characterized by linear deposits along GBM & TBM with kappa>lambda deposits in LCDD (light chain variant) and IgG in HCDD (heavy chain). EM shows powdery deposits in inner GBM, outer TBM and in the nodules.
Fibrillary and Immunotactoid GN have diffuse a proliferative GN/MPGN pattern, sometimes with crescents. They stain with PAS & silver as well, a feature they share with DN. IF is positive for polyclonal IgG and C3 in Fibrillary GN. The immunotactoid variant has monoclonal IgG with kappa/lambda chains. EM shows large, randomly arranged fibrils (16-20 nm in diameter) in the former, and parallel arrayed microtubules (20-50 nm diameter) in the latter.
 Fibronectin glomerulopathy is characterized by nodules positive with PAS and negative with silver. EM shows sub-endothelial electron dense deposits. Immunohistochemistry staining for fibronectin is diagnostic.
Fibronectin glomerulopathy is characterized by nodules positive with PAS and negative with silver. EM shows sub-endothelial electron dense deposits. Immunohistochemistry staining for fibronectin is diagnostic.
The last differential is Idiopathic Nodular Glomerulosclerosis. This entity resembles DN in all aspects except that patient is non diabetic. It is associated with long standing hypertension and smoking. Smoke contains glycation adducts which form AGEs and through oxidative stress is thought to create pathology similar to diabetes.
Thus, a nodule in the glomerulus has a wide differential with definite need for various stains, IF and EM to establish the final diagnosis. The other key feature here is most of the above mentioned diseases can have a similar clinical presentation in the same age group.
Post by Sriram Sriperumbuduri (Images from Paul Phelan)


Thank u for sharing