Jessica Faulkner, PhD
Postdoctoral Fellow
Augusta University
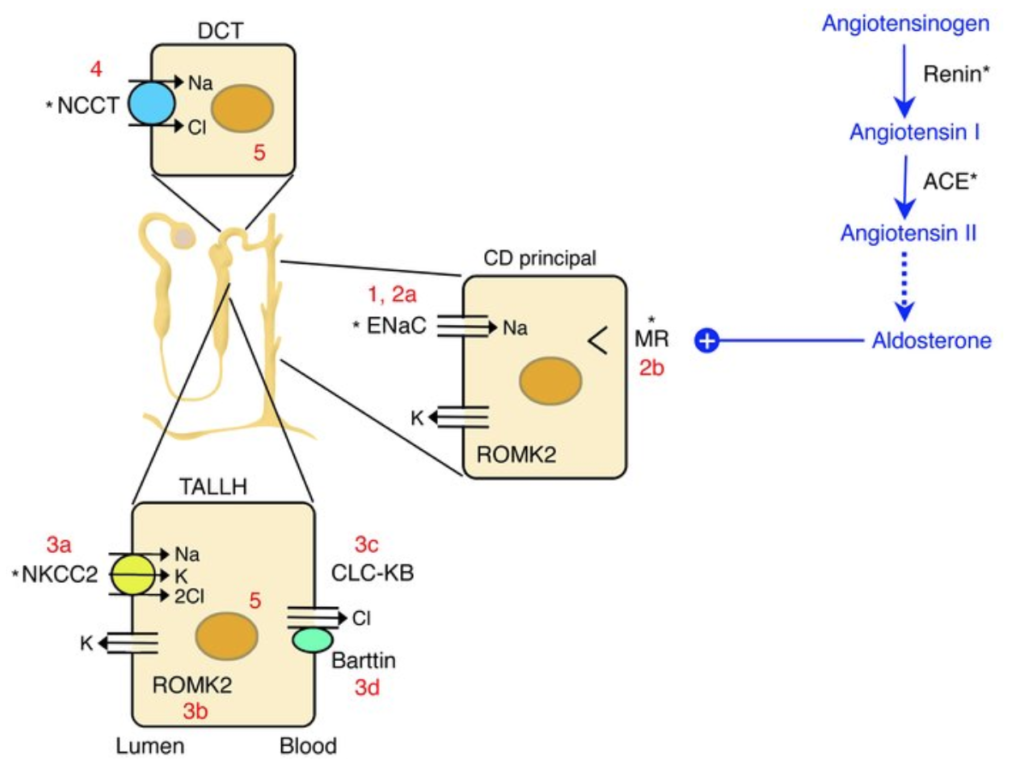
Aldosterone production and mineralocorticoid receptor (MR) activation is a key physiological pathway promoting retention of salt and water in the distal nephron. Aldosterone is a physiological ligand of MR and MR activation leads to increased epithelial sodium channel (ENaC) expression and sodium retention in the collecting duct. This pathway is a “last ditch” potent mechanism via which sodium excretion is prevented at the nephron’s final turn. Aldosterone release from the adrenal glands is stimulated in part by angiotensin II (AngII), and collectively this system is called the renin-angiotensin-aldosterone system (RAAS). Activation of the RAAS pathway contributes to sodium and volume retention, and as such is activated during times of volume depletion. Aldosterone levels characteristically increase in response to volume depletion and during a sodium depleted diet, a physiological protective response to aid in conservation of sodium and volume in an effort to maintain blood pressure. Although aldosterone is a crucial mechanism to maintain volume homeostasis, inappropriately high aldosterone levels are associated with heightened cardiovascular risk, notably increased risk of hypertension. This is evident in that MR antagonists are FDA approved therapeutics for hypertensive patients, although these agents are not currently first-line treatment options. Emerging evidence indicates, however, that targeting MR activation for blood pressure control may be a more efficacious treatment approach for certain populations, notably younger women at risk of hypertension.
Sex differences in aldosterone production
Evolutionary roles for aldosterone production and MR activation may vary between the sexes as well as with menopausal status in women. A recent study indicates that aldosterone production is heightened in premenopausal women. In a subset of patients from the HYPERPath cohort, an ongoing multi-center >1500 patient study of hypertension risk factors and outcomes, Shukri et al. (Hypertension. 2018) performed a study in which they infused AngII (3 ng/kg per min for 40 min) into
- Premenopausal aged women and age-matched men (<51 years of age)
- Women and men >51 years of age
Infusion of AngII led to higher aldosterone production in premenopausal aged women compared to postmenopausal aged women. Only premenopausal aged women demonstrated a sex difference (among men and women <51 years of age) in aldosterone response following AngII infusion, favoring a higher production in women. In addition, our lab has performed studies investigating sex differences in aldosterone production between male and female mice in response to changes in dietary sodium. We showed that on a high salt diet (4% NaCl), female mice increase adrenal CYP11B2 (the aldosterone synthase enzyme) expression and do not suppress plasma aldosterone, in contrast to male mice. In addition, we have data indicating that female mice on a sodium restricted diet (0.05% NaCl) increase adrenal CYP11B2 expression and plasma aldosterone levels more so than male mice. These data collectively indicate that females maintain higher plasma aldosterone levels than male mice at any dietary salt intake. Given that these mice studies were performed in young actively cycling female mice, these data add credence to the concept that premenopausal aged women are more predisposed to increase aldosterone production in response to stimuli compared to either males or postmenopausal women.
These data beg the question of why women evolved to better sustain plasma aldosterone levels than men during their premenopausal ages. A potential explanation may be that heightened aldosterone production in women evolved to protect sodium and water balance in pregnancy, a physiological state in which volume expansion is drastically increased. Pregnancy onset increases aldosterone production throughout gestation in association with the physiological demands of the growing feto-placental unit. Therefore, premenopausal aged women may have evolved mechanisms to protect them from decreases in aldosterone levels in response to insufficient dietary sodium intake. The mechanisms via which premenopausal aged women produce higher aldosterone levels in response to sodium depletion are the source of ongoing study.
Dysregulation of aldosterone may increase hypertension risk in premenopausal aged women
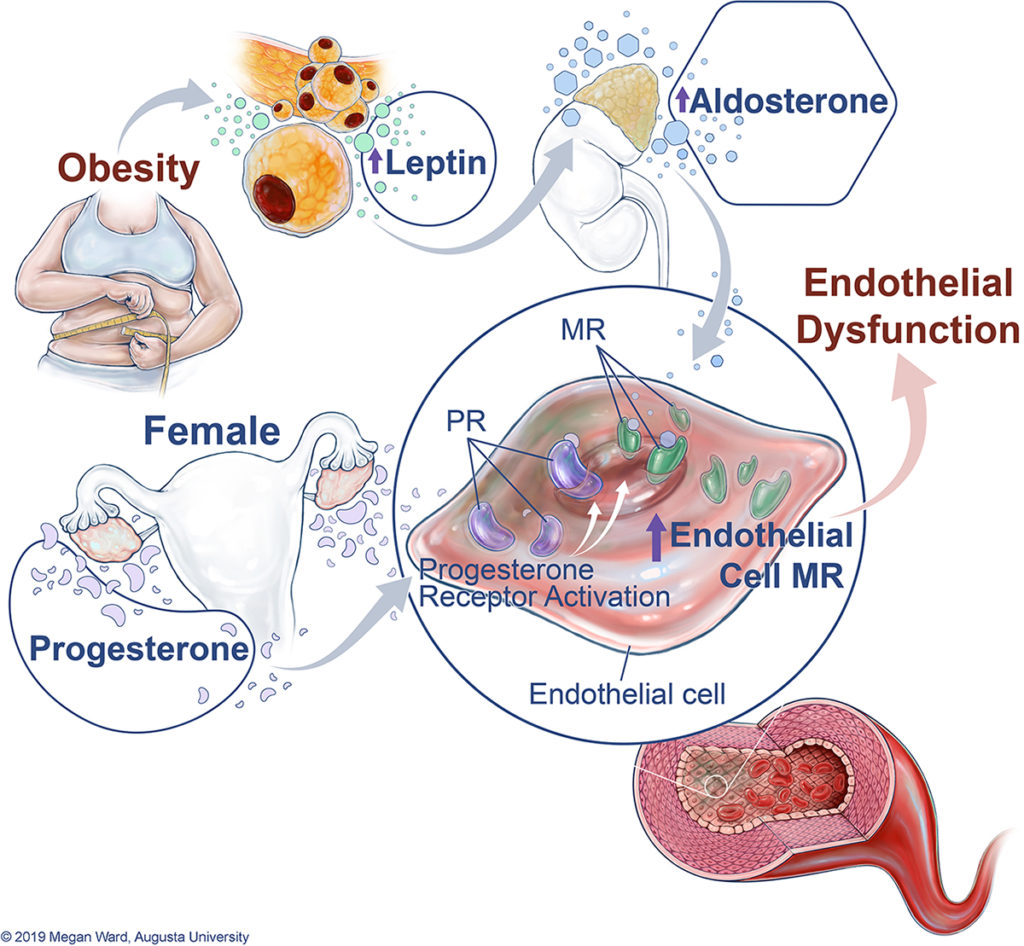
Today’s dietary environment, in which caloric and sodium intake exceeds physiological need, creates a perfect storm for reproductive aged women to be more predisposed to aldosterone-mediated pathologies. Aldosterone levels are more likely to be higher in obese and salt sensitive women than in men, both states of heightened hypertension risk. One mechanism by which this increased risk of hypertension in obese women may be occuring is via the adipocyte-derived hormone leptin. Leptin is a hormone secreted from adipose tissue that decreases appetite via activation of hunger control centers in the hypothalamus. Increased adipose tissue in obesity leads to increased plasma leptin levels. In addition, leptin deficient female animals and humans are infertile via mechanisms that are still being explored. Therefore, leptin is emerging in the literature as a reproductively-tied hormone in women. Our lab has also shown that leptin induces an increase in aldosterone production via increasing CYP11B2 expression in the adrenal glands. Currently, roughly ⅔ of premenopausal aged women are overweight or obese, both of which are associated with elevated plasma aldosterone levels. These women are likely at heightened risk of aldosterone-mediated hypertension risk in the current dietary environment. In addition to sustained aldosterone production, premenopausal aged women may be more sensitive to aldosterone-mediated hypertension via an increased sensitivity of the vascular endothelium to MR activation. Although aldosterone is a potent sodium retention hormone via MR activation in the collecting duct, MRs are expressed in many tissue types. Emerging experimental evidence indicates that the endothelial cell specific MR is a critical mediator of endothelial function and vascular tone in female mice. Endothelial MR activation induces the production of inflammatory cytokines, reactive oxygen species and serves to decrease endothelial relaxation responses. Our data shows that endothelial MR expression is endogenously elevated in female mice and humans compared to males, which is stimulated by higher progesterone levels in females. Additionally, we demonstrated in this report that pregnant mice exhibit an upregulation of endothelial MR expression in association with high progesterone levels in pregnancy. Given that progesterone is the predominant female sex hormone involved in fetal and placental development and maturation, these data indicate that progesterone-induced endothelial MR may play a role in pregnancy. The evolutionary need for this mechanism is speculative at present. This mechanism may be tied to the needs of the vascular endothelium to readily adapt to decreases in plasma volume in pregnancy by maintaining endothelial tone and blood flow to the growing feto-placental unit. Pregnant women with high progesterone, aldosterone and endothelial MR expression do not spontaneously develop endothelial dysfunction due to the onset of vasoprotective mechanisms (reduced endothelin-1 expression, increases in systemic nitric oxide bioavailability). However, obese or salt sensitive women are likely at heightened risk for endothelial dysfunction due to higher aldosterone and higher endothelial MR expression. Emerging clinical evidence indicates that endothelial dysfunction is a critical mediator of hypertension in women, therefore, heightened endothelial MR activation may predispose women to higher blood pressures.
MR antagonists may be more efficacious for non-pregnant, premenopausal women with hypertension
The advent of spironolactone, the first widely available MR antagonist, demonstrated that MR blockade decreased blood pressure. However, spironolactone’s off-target anti-androgenic effects, in addition to the advent of newer therapeutics such as ACE inhibitors, saw the drug fall out of favor as a first-line hypertension treatment. Recent clinical and experimental data has brought MR antagonists, especially the newer and more specific MR antagonists eplerenone and finerenone, to a conversation of their use in personalized medicine approaches for female patients. Emerging clinical studies indicate that MR antagonists are more efficacious for blood pressure lowering in women than in men. Therefore, the predominance of the aldosterone-MR pathway in premenopausal aged women, particularly those with obesity or salt sensitivity, may provide a key target for the treatment of hypertension in this group. Importantly, some MR antagonists are contraindicated in pregnancy so pregnant women or those currently trying for a pregnancy may not be candidates for this line of treatment.
Reviewed by: Elinor Mannon, Kelly Hyndman, PhD, Matthew Sparks, MD, FASN, FAHA
If you enjoyed reading this post and are interested in learning more about aldosterone and its role in kidney function, consider checking out these resources on RFN:
Basic Review: The Renin-Angiotensin-Aldosterone Axis
RAAS is Your Friend: Pocket Guide to Heritable Blood Pressure Disorders

Very useful well written article. Thank you!
Best information that anyone can ever have on renal .
Excellent article
I have observed this in clinical practice. Great to understand the mechanistic correlation.