What is “isolated lipiduria”?
The detection of urinary lipid droplets with a typical Maltese cross appearance in the absence of proteinuria or albuminuria.
There are no reports or systematic analyses of this phenomenon, so this post reflects anecdotal observations. The purpose of presenting this topic here is to spark interest and promote scientific evaluation of this phenomenon, and perhaps reconsider the meaning of lipiduria.
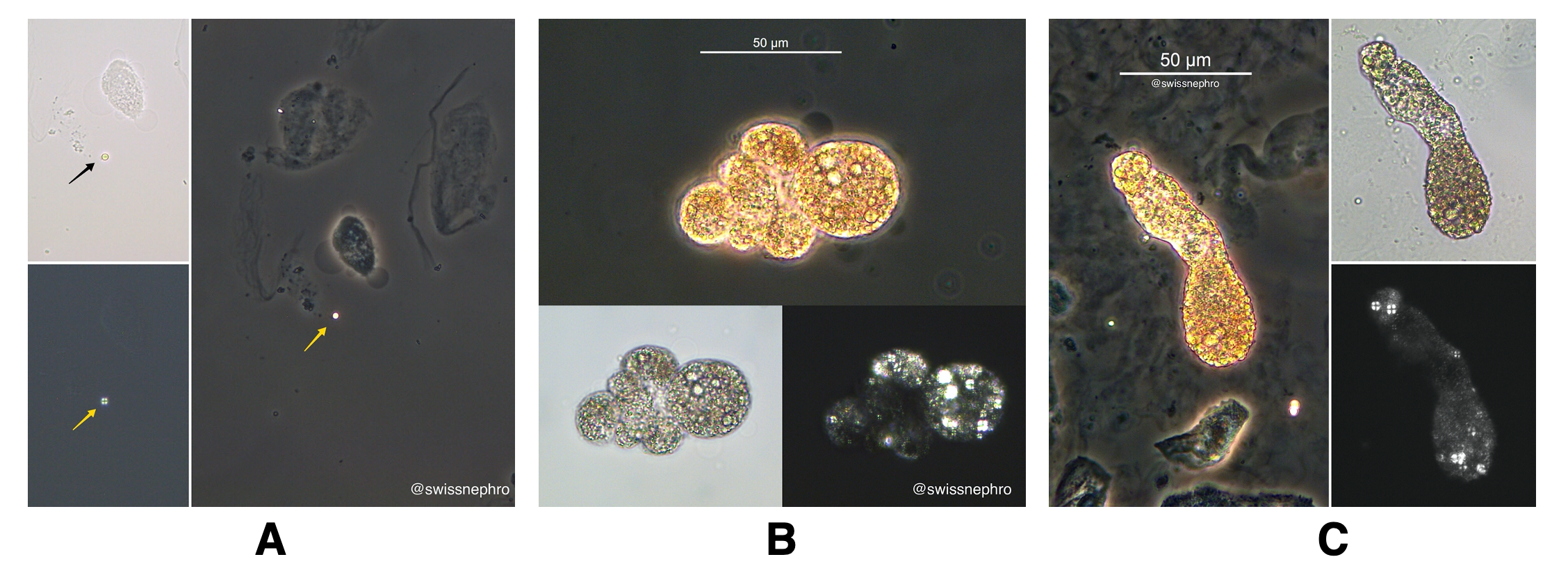
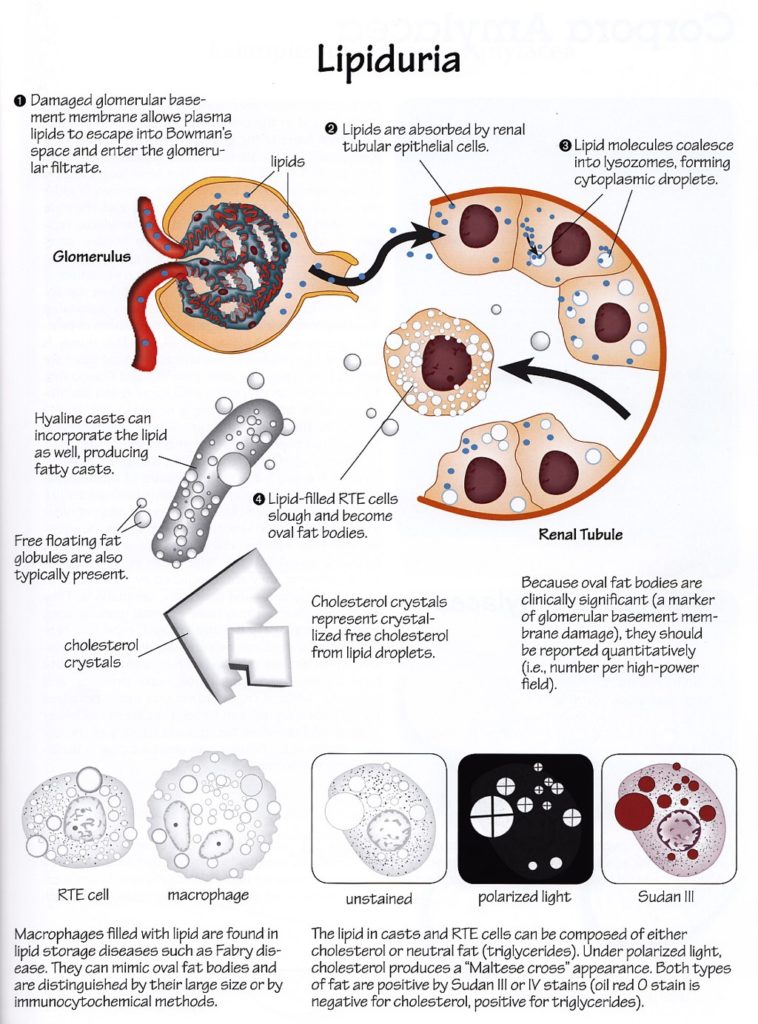
Lipiduria is a common finding in patients with higher-grade, glomerular proteinuria. Previous Renal Fellow Network posts have discussed oval fat bodies and the pathophysiology of lipiduria. It commonly refers to the presence of anisotropic lipid droplets, which are globular bodies with a typical Maltese cross appearance when viewed with a polarizing microscope (Fig. 1A). These can be seen freely or within cells (oval fat bodies, Fig. 1B) or casts (Fig. 1C).
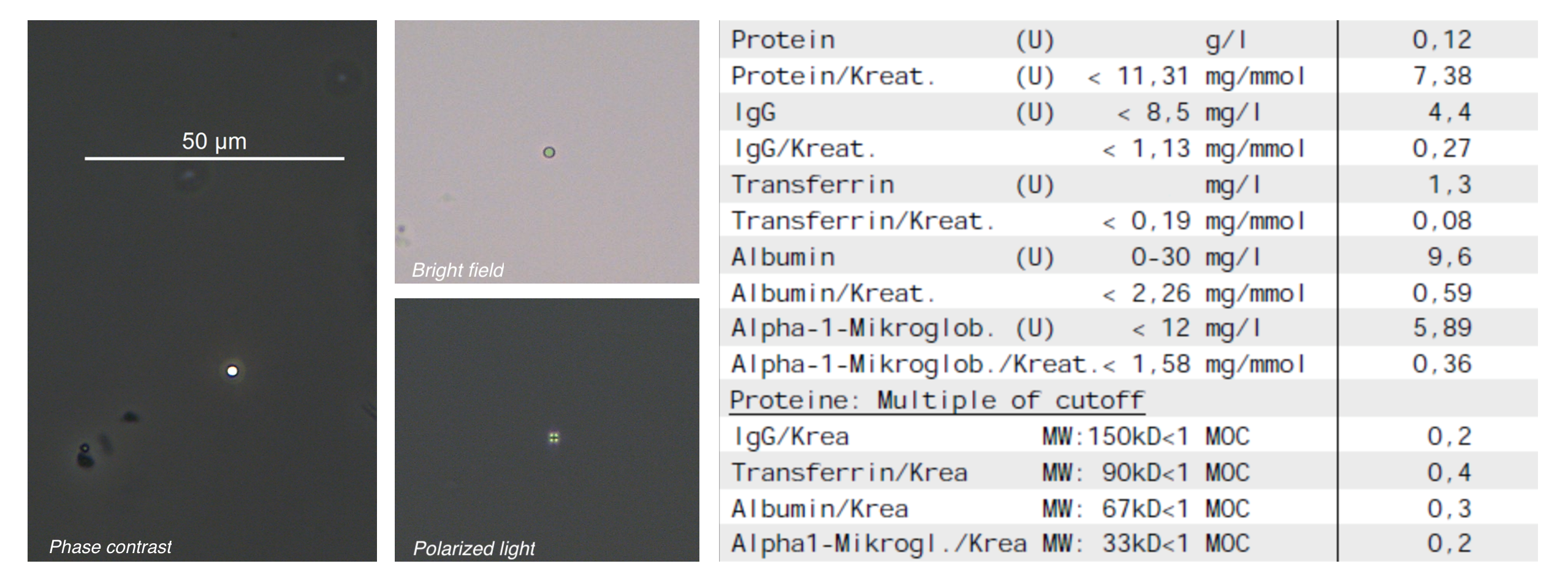
Occasionally, these particles are fund in the urine of patients without proteinuria (Fig. 2). Observed cases of isolated lipiduria share a few features:
- Scarce amounts of lipid droplets were present-less than 3 per 10 high-power fields
- No oval fat bodies or lipid casts, signs of glomerular hematuria or tubular injury were present
- Lipiduria was missed by our central laboratory which uses an automated system for initial screening of urine samples
Anecdotally, patients with isolated lipiduria had normal or near normal kidney function and had either moderate to severe hypertension or morbid adiposity. As both conditions are well-established risk factors for podocyte damage and adaptive focal segmental glomerulosclerosis (FSGS) FSGS, it is possible that isolated lipiduria is an early indicator of these disease processes. It is also possible that in these early stages there is increased glomerular filtration of high-molecular weight proteins, leading to their increased uptake into proximal tubular cells and the formation of lipid droplets. There may be a range of albumin filtration within which the increased albumin can still be mostly reabsorbed by the proximal tubule (so that there is no increase in urinary excretion of albumin) but the presence of lipid droplets still demonstrates increased glomerular permeability for protein.
Isolated lipiduria is likely a rare event – though as nephrologists do not see patients without established kidney disease and because of the fact that it is easily missed by automatic analyzer-assisted urine examination, true prevalence may be higher. Anisotropic lipid droplet identification is usually straightforward, though polarizing light is needed for confirmation. In “busy” sediments, it can be worthwhile to look for the occasional lipid droplet by screening high-power fields with polarized light directly.
These considerations rely heavily on the concept that anisotropic lipid droplets are the result of increased glomerular filtration and proximal tubular reabsorption of albumin-bound fatty acids and/or lipoproteins, followed by the metabolism or transport of these lipids into cholesterol ester containing cellular vesicles.
The necessity of a glomerular insult to produce anisotropic lipiduria has been questioned by two commonly cited papers, which describe the detection of oval fat bodies in non-glomerular kidney disease and ADPKD specifically. In both series, all patients with oval fat bodies seem to have had significant albuminuria. The lipiduria correlated with albuminuria, but not blood pressure or kidney function. Thus, the anisotropic lipiduria in patients with primarily non-glomerular kidney disease could very well be explained by secondary glomerular damage and would then be perfectly aligned with the hypothesis of lipiduria as a sign of podocyte injury.
Especially in patients with no or little albuminuria, further examination of the diagnostic and prognostic meaning of anisotropic lipiduria may be worthwhile.
Post by: Florian Buchkremer

