Welcome to the 36th case of the Skeleton Key Group, a team of nephrologists from around the world who build a periodic education package for the Renal Fellow Network.
Author: Matan Khanian MD
A. Stem
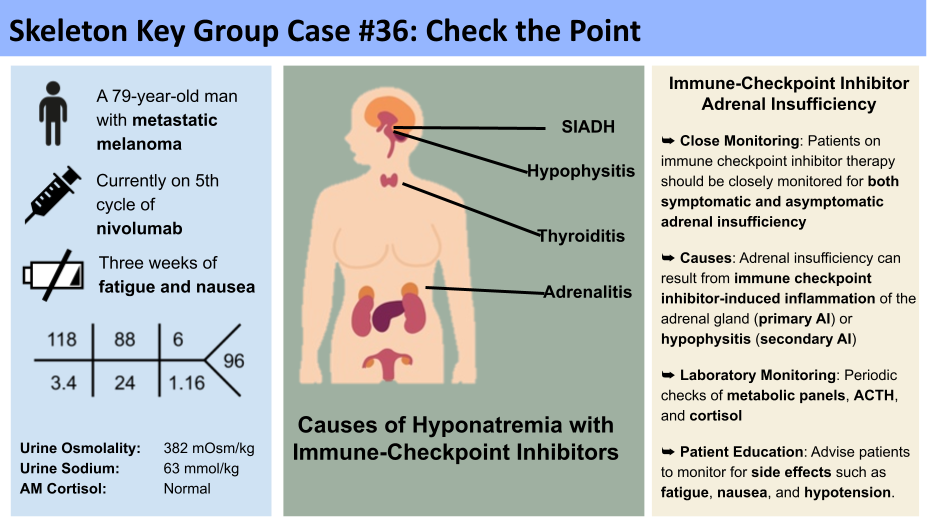
A 79-year-old man with CKD of unknown cause and metastatic melanoma presented to the emergency department with fatigue, decreased appetite, and nausea for about one week. Outpatient labs showed a serum sodium of 113 mEq/L and he was called in to the emergency department. On a repeat in the hospital, the Na was 118 mEq/L. He is currently on his 5th cycle of nivolumab, last received 3 weeks ago. Despite decreased appetite, he reported adherence to his home medications:
- Olmesartan
- Hydrochlorothiazide
- Rosuvastatin
- Tamsulosin
Upon evaluation in the emergency department:
Vital signs:
- Temperature 36.9 celsius
- Blood pressure 110/50 mm Hg
- Heart rate 82 bpm
- Respiratory rate 16
- Oxygen saturation 90% on room air
Physical examination:
General: elderly man with dry appearing oral mucosal membranes
Neck: no jugular venous distention
Heart: no murmurs
Lungs: clear to auscultation bilaterally, not in respiratory distress
Abdomen: soft, non-tender, non-distended
Skin: visible skin tenting
Extremities: no lower extremity edema
B. Labs

Serum osm: 242 mOsm/Kg
Urine osm: 214 mOsm/kg
Urine sodium: 61 mmol/L
TSH: 8.94 ulU/ml
FT4 <0.2 ng/dL
Morning Cortisol: 2.9 ug/dl
C. Workup
Hyponatremia in a patient with cancer
Hyponatremia is commonly seen in patients with cancer due to many potential factors, including poor nutritional intake, volume depletion, and paraneoplastic syndromes (Table 1). Hyponatremia in patients with cancer often signifies advanced disease and is associated with increased mortality. Additionally, many cancer-related therapies contribute to the development of hyponatremia. Traditional chemotherapy agents, including vincristine, vinblastine, and cyclophosphamide, are also implicated in hyponatremia primarily through mechanisms such as the syndrome of inappropriate antidiuretic hormone. Monoclonal antibodies, immunomodulators like interferon and interleukin-2, and newer targeted therapies have also been associated with hyponatremia. Immune checkpoint inhibitors, such as nivolumab, are increasingly recognized as a cause of hyponatremia.

Table 1 derived from: Potential causes of hyponatremia in cancer. From: Kitchlu A, Rosner MH. Hyponatremia in patients with cancer. Curr Opin Nephrol Hypertens. 2019;28(5):433-440.
The Evaluation
The initial workup of hyponatremia starts with obtaining a serum osmolality to determine if it is a true hypoosmolar hyponatremia. If hypoosmotic hyponatremia is confirmed, this is followed by urine osmolality to assess for antidiuretic hormone (ADH) activity and urine Na to tell us about renin-angiotensin-aldosterone system (RAAS) activity. (See our previous SKG Case #24 and Case #32 for a more detailed review of the evaluation of hyponatremia).

In this case, the patient presented with a sodium level of 118 mEq/L, serum osmolality of 242 mOsm/Kg, urine osmolality of 214 mOSM/kg and urine sodium level of 61 mmol/L. This represents a hypoosmotic (serum osm < 285 mOsm/kg) hyponatremia (serum sodium < 135 mL/min) with relatively increased ADH activity (urine osm >100 mOsm/Kg) and suppressed RAAS activity (urine Na > 30 mEq/L). But before we blame this on the Syndrome of Inappropriate Antidiuretic Hormone, we must evaluate for other causes of inappropriately high ADH activity such as adrenal insufficiency or hypothyroidism. It is important to note that SIADH is often a diagnosis of exclusion and initial workup of hyponatremia should remain broad; for example, the urine sodium could be elevated from diuretics, metabolic alkalosis, sodium wasting from adrenal insufficiency, etc. Past medical history, medication list, laboratory studies and imaging may help with the diagnosis.
In this case, further testing revealed a fasting cortisol level of 2.9 ug/dl (4.0-22.0 ug/dl) and an inappropriately low adrenocorticotropic hormone (ACTH) of 7.5 pg/mL (7.2-63 pg/mL). The low morning cortisol level made adrenal insufficiency (AI) the most likely diagnosis. Adrenal insufficiency can result from immune checkpoint inhibitor-induced inflammation and antibodies attacking the adrenal gland (primary AI) or pituitary gland causing hypophysitis (secondary AI). An ACTH stimulation test can help differentiate this by assessing the adrenal glands ability to produce cortisol in response to synthetic ACTH. In primary AI, the adrenal glands are damaged and unable to produce sufficient cortisol even with ACTH stimulation, resulting in a suboptimal cortisol response. Secondary AI due to hypophysitis involves impaired ACTH secretion from the pituitary gland, but the adrenal glands retain the ability to respond to prolonged ACTH stimulation.
Adrenal insufficiency leads to decreased aldosterone, cortisol and androgen production. Cortisol normally inhibits ADH secretion. A cortisol deficiency (primary and secondary AI) leads to excess ADH secretion causing water retention and hyponatremia. Moreover, lack of cortisol and aldosterone (primary AI but not secondary AI) will lead to lower blood pressures, further increasing ADH activity and contributing to hyponatremia. (See our recent SKG Case #34 to review the mechanisms by which primary vs secondary adrenal insufficiency causes hyponatremia). This patient was also found to have a TSH 8.94 uIU/ml ( 0.34-4.82 uIU/ml), fT4 < 0.20 ng/dL (0.59-1.80 ng/dL), also confirming hypothyroidism. TRH and CRH were ordered but canceled by the lab due to insufficient volume.
Electrolyte and Acid-base disturbances associated with immune checkpoint inhibitors (ICIs).Table adapted from Uppal et al.

D. Diagnosis
Given the patient’s history of checkpoint inhibitor therapy, which is a potential cause of both adrenal insufficiency and thyroid dysfunction, along with the laboratory findings of isolated ACTH deficiency, we went ahead and began treatment with hydrocortisone. The patient clinically responded quickly to treatment with hydrocortisone, thus supporting the diagnosis of secondary hypophysitis adrenal insufficiency in setting of checkpoint inhibitor use.

Figure: Nivolumab stimulates T cells memory response by preventing tumor cells from triggering PD-1. From: Guo L, Zhang H, Chen B. Nivolumab as Programmed Death-1 (PD-1) Inhibitor for Targeted Immunotherapy in Tumor. J Cancer. 2017;8(3):410-416.
Nivolumab is an anti-programmed cell death monoclonal antibody which prevents the binding of PD-1 to its ligands PD-L1 and PD-L2 in stimulating memory response to tumor antigen-specific T cell proliferation. However, this process can also result in an unchecked immune response that manifests in the form of autoimmune-like or inflammatory adverse effects. Of note, the most common kidney adverse event associated with checkpoint inhibitors is acute kidney injury due to interstitial nephritis. Among non-kidney related adverse events associated with checkpoint inhibitors (both Anti-PD-1 and Anti -CTLA-4), the most common is hypothyroidism. But these autoimmune-like manifestations can occur in almost every organ, leading to potential dermatitis, pneumonitis, colitis, esophagitis, adrenal insufficiency, or myositis. The most serious and life-threatening complications of checkpoint inhibitors include adrenal crisis, hypophysitis, immunotherapy-related colitis, Triple M syndrome, Stevens-Johnson syndrome, or toxic epidermal necrolysis.
Routine screening for adrenal insufficiency while on nivolumab therapy is not recommended by current guidelines. However, many cases of immune checkpoint inhibitor adrenal insufficiency have been reported. This could in part be due to difficulty in establishing a diagnosis. Adrenal insufficiency often presents with vague and non-specific symptoms which may go unrecognized. Moreover, a single ACTH level is insufficient. Rather, an accurately timed morning cortisol level, in conjunction with ACTH and possibly even ACTH stimulation testing are needed to confirm this diagnosis.
E. Followup
The patient was started on hydrocortisone 50 mg Q8 hours, levothyroxine 50 mcg daily, as well as 100 ml/hr normal saline. A fluid restriction of 1 L per day with a goal sodium correction of 6 mEq/L in the first 24 hours. Throughout his stay his sodium corrected to 122 mEq/L within 24 hours, and subsequently improved to 134 by day 5 of hospitalization. The patient was continued on high-dose hydrocortisone and had return of his appetite and resolution of the fatigue. The hydrocortisone was tapered to 20 mg qAM and 10 mg nightly on day three. The following day he was lethargic, hypoxic, and in shock with a systolic blood pressure in the 50s and he was started on norepinephrine and an extra dose of hydrocortisone. The infectious workup was negative, suggesting too rapid titration of steroids. The patient underwent a slower taper of hydrocortisone and was discharged home.
F. Take home points:
- Hyponatremia is common in patients with advanced cancers, and the differential diagnosis should include adverse effects of anti-cancer drugs
- Patients with cancer on immune checkpoint inhibitor therapy should be closely monitored for both symptomatic and asymptomatic adrenal insufficiency, which can lead to hyponatremia
- Adrenal insufficiency can result from immune checkpoint inhibitor-induced inflammation of the adrenal gland (primary AI) or hypophysitis (secondary AI)
- Patients on immune checkpoint inhibitors may benefit from periodic metabolic panels to monitor for electrolyte derangements such as hyponatremia, as well as monitoring of cortisol and ACTH levels
- Patients should also be advised of such side effects and to be monitored for symptoms of adrenal insufficiency such as hypotension and fatigue.
Editors: Jefferson L. Triozzi, Raad B. Chowdhury, Payal Gaggar, Chi Chu, Joel Topf, Matthew A. Sparks