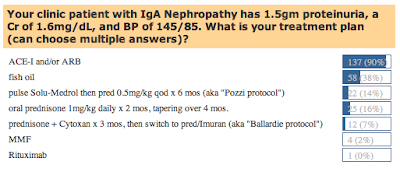
The results of last week’s poll on IgA Nephropathy are in: 90% of individuals correctly identified that the only treatment shown in randomized controlled trials to consistently benefit patients with IgA Nephropathy is ACE-inhibitors and/or ARBs. The response was pretty divided beyond that, however, with a variable number of individuals (37% in all) opting for a trial of immunosuppression. In retrospect, I’ll admit that the question was not perfectly worded: whether the patient has already been treated with ACE-I/ARB therapy was not really clear. If the patient is just recently diagnosed with IgA Nephropathy, a case could be made to avoid immunosuppression initially and to see whether or not ACE-I/ARB therapy alone could suppress proteinuria and hypertension to acceptable levels. According to this review in Brigham & Women’s “Nephrology Rounds” from 2007, a trial of steroids or possibly even more aggressive cytotoxic therapy (e.g., cyclophosphamide) could be attempted in an individual with these lab parameters who is not responding to conservative therapy. A majority of folks said they would use fish oil, a topic which has been covered previously.
 This week’s RFN Poll question is a fun one: let’s assume Obama’s stimulus package includes in its budget funding for a “Mount Rushmore of Nephrology” to be built. This gigantic statue will feature the faces of 4 prominent nephrologists etched into the rock face of a majestic mountain, preferably at one of the national parks in the Western United States. Of all the prominent nephrologists, which four would you choose as being the most influential in the field? Choose from the list of historic figures listed, and feel free to include “write-in votes” under the “comments” section if your favorite nephrologist is not listed. The list I made is admittedly biased towards physicians who have been practicing recently enough that the subspecialty has actually been in existence (e.g., not including folks like Hippocrates), and conversely I tended not to include the current heavy hitters of Nephrology, reasoning that the jury is still out on these folks. Realize that this is for fun, and I’m sure I’ve made several oversights.
This week’s RFN Poll question is a fun one: let’s assume Obama’s stimulus package includes in its budget funding for a “Mount Rushmore of Nephrology” to be built. This gigantic statue will feature the faces of 4 prominent nephrologists etched into the rock face of a majestic mountain, preferably at one of the national parks in the Western United States. Of all the prominent nephrologists, which four would you choose as being the most influential in the field? Choose from the list of historic figures listed, and feel free to include “write-in votes” under the “comments” section if your favorite nephrologist is not listed. The list I made is admittedly biased towards physicians who have been practicing recently enough that the subspecialty has actually been in existence (e.g., not including folks like Hippocrates), and conversely I tended not to include the current heavy hitters of Nephrology, reasoning that the jury is still out on these folks. Realize that this is for fun, and I’m sure I’ve made several oversights. 

Great suggestions. I'm sure I've missed many more.
Ed Lewis, most important clinical work on ACE and ARB in DM
I would like to add a few names
1. Thomas E. Andreoli- First division chief at UAB, past editor of kidney international, editor of cecils essentials of medicine, past ASN and ISN president. Authority on water metabolism and mechanism of amphotericin nephrotoxicity.
2. Steve Hebert- cloning of the ROMK channel, calcium sensing receptor, NCC and NKCC2.
I could go on, but will stop here.
Matt Sparks