Lithium is indispensable as an effective treatment for
bipolar affective disorder. However, it has a narrow therapeutic index with
desired therapeutic levels between 0.6 and 1.2 mEq/L. Lithium is handled by the kidney (responsible for almost all its
excretion) in a manner very similar to sodium. It has a molecular weight of 7
daltons, has a moderate volume of distribution, is <10% protein bound and is therefore readily
dialyzable. Lithium may
cause of myriad of renal related toxicities, some of which are classic
descriptions and some which are less well known. Much of this has been
discussed on RFN before (here, here) but I felt a refresher with some additions
was due.
Nephrogenic Diabetes Insipidus (NDI)
This is perhaps the best know and most common complication
of lithium therapy, with an estimated prevalence of 20-70%. Patients
present with polyuria and polydipsia due to a urinary concentrating defect that
can lead to volume depletion, especially if access to free water is restricted.
Lithium downregulates aquaporin-2, vasopressin-activated water channels expressed
on the collecting duct principal
cells. It is worth noting that ongoing volume depletion from NDI may aggravate
the risk of supra-therapeutic levels and therefore chronic nephrotoxicity.
Amiloride may help as it inhibits lithium reabsorption via ENaC in the
collecting duct.
of lithium therapy, with an estimated prevalence of 20-70%. Patients
present with polyuria and polydipsia due to a urinary concentrating defect that
can lead to volume depletion, especially if access to free water is restricted.
Lithium downregulates aquaporin-2, vasopressin-activated water channels expressed
on the collecting duct principal
cells. It is worth noting that ongoing volume depletion from NDI may aggravate
the risk of supra-therapeutic levels and therefore chronic nephrotoxicity.
Amiloride may help as it inhibits lithium reabsorption via ENaC in the
collecting duct.
Renal tubular Acidosis (RTA)
Lithium
may induce a hyperchloremic non-anion gap metabolic acidosis, analogous to
a distal RTA. It is likely due to decreased distal proton secretion. Unlike
acidosis associated with amiloride, it is not associated with hyperkalemia
probably because of their different effects on distal H+/K+-ATPase
function.
may induce a hyperchloremic non-anion gap metabolic acidosis, analogous to
a distal RTA. It is likely due to decreased distal proton secretion. Unlike
acidosis associated with amiloride, it is not associated with hyperkalemia
probably because of their different effects on distal H+/K+-ATPase
function.
Acute Lithium Nephrotoxicity
This may occur as an overdose in newly treated patients or
those on long-term lithium therapy. Acute lithium intoxication may cause altered mental status
and acute kidney injury. Drugs which decrease GFR (NSAIDs/RAAS inhibitors) may exacerbate
intoxication as can thiazides, which cause a natriuresis and a subsequent reabsorption
of Na (and lithium). With preserved renal function and mild intoxication, increasing
urine output/forced diuresis may be all that is needed. Care should be taken
using 0.9%NaCl if hypernatremia from NDI is present. As mentioned above, lithium is readily dialyzable and
hemodialysis (ideally using a high flux membrane to aid clearance) is the primary
management for severe cases. A lithium level >4mEq/L is considered an
absolute indication for dialysis in most cases. A level >2.5mEq/L with severe
symptoms, or renal impairment which will slow native clearance, is also an
indication. If in doubt, most nephrologists would have a low threshold for
dialysis, although it is usually not needed with a level <2.5mEq/L. Drug
levels drop rapidly during dialysis but they do rebound so extended and
repeated sessions are usually necessary. Continuous therapies are less efficient
so are not desirable if severe intoxication is present but may be used if
conventional dialysis is not immediately available.
those on long-term lithium therapy. Acute lithium intoxication may cause altered mental status
and acute kidney injury. Drugs which decrease GFR (NSAIDs/RAAS inhibitors) may exacerbate
intoxication as can thiazides, which cause a natriuresis and a subsequent reabsorption
of Na (and lithium). With preserved renal function and mild intoxication, increasing
urine output/forced diuresis may be all that is needed. Care should be taken
using 0.9%NaCl if hypernatremia from NDI is present. As mentioned above, lithium is readily dialyzable and
hemodialysis (ideally using a high flux membrane to aid clearance) is the primary
management for severe cases. A lithium level >4mEq/L is considered an
absolute indication for dialysis in most cases. A level >2.5mEq/L with severe
symptoms, or renal impairment which will slow native clearance, is also an
indication. If in doubt, most nephrologists would have a low threshold for
dialysis, although it is usually not needed with a level <2.5mEq/L. Drug
levels drop rapidly during dialysis but they do rebound so extended and
repeated sessions are usually necessary. Continuous therapies are less efficient
so are not desirable if severe intoxication is present but may be used if
conventional dialysis is not immediately available.
Chronic Tubulointerstitial Nephritis (TIN)
A chronic TIN with interstitial fibrosis and tubular dropout
is the commonest pathology seen when patients with lithium and renal impairment
are biopsied. Consistent with this is a bland urine sediment with little/no
proteinuria being common (although not exclusive-see next section). As
nephrologists, our view of the prevalence of lithium induced CKD is skewed. The
exact prevalence is difficult to determine but many patients have preserved
renal function. The tricky decision is whether (and if so when) to stop therapy?
This is rarely a decision the nephrologist can make alone and should be balanced
with efficacy of treatment/alternatives available and usually led by the psychiatrist
in my opinion.
is the commonest pathology seen when patients with lithium and renal impairment
are biopsied. Consistent with this is a bland urine sediment with little/no
proteinuria being common (although not exclusive-see next section). As
nephrologists, our view of the prevalence of lithium induced CKD is skewed. The
exact prevalence is difficult to determine but many patients have preserved
renal function. The tricky decision is whether (and if so when) to stop therapy?
This is rarely a decision the nephrologist can make alone and should be balanced
with efficacy of treatment/alternatives available and usually led by the psychiatrist
in my opinion.
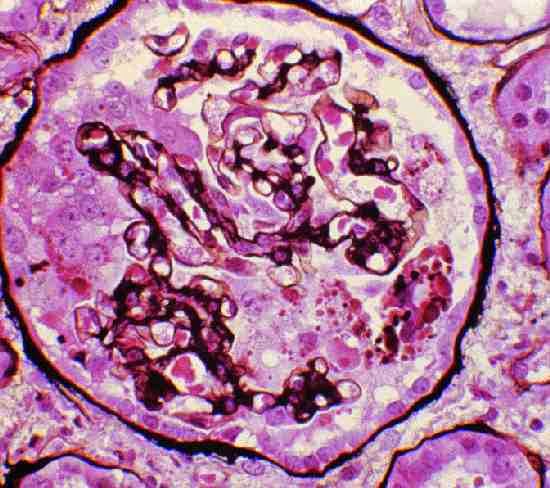
Nephrotic Syndrome
It is less well known that lithium may be associated with a
glomerulopathy. Minimal change disease is most often described but membranous
nephropathy and FSGS has also been reported. Cases were considered lithium induced as proteinuria disappeared upon cessation of the drug, and when re-challenged (for psychiatric reasons), the nephrotic syndrome recurred. A series of 24 patients with
lithium-induced nephrotoxicity from New York included one quarter with
nephrotic-range proteinuria. My initial thoughts were that the FSGS lesions were likely secondary
to nephron loss and resulting hyperfiltration injury. However, arguing against
this is that presence of FSGS lesions did not correlate with severity of tubulointerstitial
lesions. Moreover, there was a high incidence of extensive podocyte foot process
effacement, to a degree uncommon in secondary FSGS. The mechanism of glomerular toxicity is unclear.
glomerulopathy. Minimal change disease is most often described but membranous
nephropathy and FSGS has also been reported. Cases were considered lithium induced as proteinuria disappeared upon cessation of the drug, and when re-challenged (for psychiatric reasons), the nephrotic syndrome recurred. A series of 24 patients with
lithium-induced nephrotoxicity from New York included one quarter with
nephrotic-range proteinuria. My initial thoughts were that the FSGS lesions were likely secondary
to nephron loss and resulting hyperfiltration injury. However, arguing against
this is that presence of FSGS lesions did not correlate with severity of tubulointerstitial
lesions. Moreover, there was a high incidence of extensive podocyte foot process
effacement, to a degree uncommon in secondary FSGS. The mechanism of glomerular toxicity is unclear.
Renal Cell Tumors
It has recently been reported in Kidney International that
chronic lithium use is associated with an increased risk of kidney
tumours. After a mean duration of lithium
exposure of >21 years, patients had a significantly higher risk of solid
renal tumours compared with gender, age and eGFR matched controls [Standardized
Incidence Ratio i.e. ratio of
observed-to-expected numbers of renal cancers was 7.51 and 13.69 in men and
women respectively]. The tumours were a mixed bag of benign (oncocytomas,
angiomyolipomas etc.) and malignant (clear cell, stromal, papillary) lesions.
While these results are thought provoking, this was a retrospective study and
the design seems open to detection bias in my opinion (were patients on lithium
screened more than regular individuals?).
chronic lithium use is associated with an increased risk of kidney
tumours. After a mean duration of lithium
exposure of >21 years, patients had a significantly higher risk of solid
renal tumours compared with gender, age and eGFR matched controls [Standardized
Incidence Ratio i.e. ratio of
observed-to-expected numbers of renal cancers was 7.51 and 13.69 in men and
women respectively]. The tumours were a mixed bag of benign (oncocytomas,
angiomyolipomas etc.) and malignant (clear cell, stromal, papillary) lesions.
While these results are thought provoking, this was a retrospective study and
the design seems open to detection bias in my opinion (were patients on lithium
screened more than regular individuals?).
Hyperparathyroidism
As previously posted, lithium may cause hypercalcemia and stimulate
PTH via a variety of postulated mechanisms (see previous post).
PTH via a variety of postulated mechanisms (see previous post).