 At renal grand rounds this week, I presented a case of a
At renal grand rounds this week, I presented a case of agentleman who presented with fevers, confusion, and lower extremity pain during
dialysis. The patient would spike low grade fevers pre-HD and then fevers up to
105 post-HD. He had a tunneled HD line, but blood cultures were negative, and
his fevers persisted in spite of changing the line. We were initially concerned
for a dialyzer membrane reaction, but the time course of fevers was not
consistent with either type A or type B reaction, and his symptoms persisted
even after switching to an Exceltra membrane. The patient was worked up
further, and his serum electrophoresis revealed 2 M components, serum free
light chains showed an elevated Kappa/Lambda ratio, and he had a positive urine
Bence Jones protein. His CH50 and C4 levels were undetectable, but C3 was only
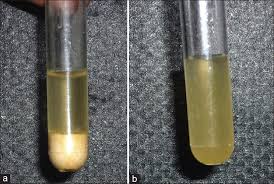
mildly low. Cryocrit was sent, and was positive for a type 2 cryoprotein with a
predominant IgM Kappa component.
It was unclear why the symptoms of cryoglobulinemia
worsened with dialysis; it was hypothesized that hemoconcentration with
ultrafiltration, along with exposure of blood to cooler temperatures within the
dialysis tubing led to transient complement consumption and an inflammatory
reaction. The symptoms of mixed cryoglobulinemia are typically nonspecific, and
patients usually present with arthralgias, fatigue, palpable purpura, and
peripheral neuropathy. C4 and total complement are usually dramatically low, as
in this case.
worsened with dialysis; it was hypothesized that hemoconcentration with
ultrafiltration, along with exposure of blood to cooler temperatures within the
dialysis tubing led to transient complement consumption and an inflammatory
reaction. The symptoms of mixed cryoglobulinemia are typically nonspecific, and
patients usually present with arthralgias, fatigue, palpable purpura, and
peripheral neuropathy. C4 and total complement are usually dramatically low, as
in this case.
Treatment of cryoglobulinemia usually involves the use of
plasmapheresis to remove circulating cryoglobulins. Steroids are suppressive in
some patients, and rituximab quells formation of new cryoglobulins. There
are no studies aside from case reports about the use of eculizumab for
cryoglobulinemia. Trendelenburg et al analyzed the role of complement in
glomerular inflammation using mice models, and showed that mice deficient in C5
had reduced glomerular infiltration by neutrophils. Eculizumab inhibits the
conversion of C5a to C5b and subsequent formation of the membrane attack
complex; it therefore be theoretically useful in treating cryoglobulinemia,
which causes complement mediated renal failure.
plasmapheresis to remove circulating cryoglobulins. Steroids are suppressive in
some patients, and rituximab quells formation of new cryoglobulins. There
are no studies aside from case reports about the use of eculizumab for
cryoglobulinemia. Trendelenburg et al analyzed the role of complement in
glomerular inflammation using mice models, and showed that mice deficient in C5
had reduced glomerular infiltration by neutrophils. Eculizumab inhibits the
conversion of C5a to C5b and subsequent formation of the membrane attack
complex; it therefore be theoretically useful in treating cryoglobulinemia,
which causes complement mediated renal failure.
The patient was treated with 2 doses of eculizumab and
then rituximab for cryoglobulinemia, and is now doing well and tolerating
dialysis.
then rituximab for cryoglobulinemia, and is now doing well and tolerating
dialysis.
Posted by Shruti Gupta, Renal Fellow MGH/BWH

