Our last post on lupus nephritis focused on pathogenesis ,clinical presentation, grading and class I/II disease. The next segment this month will cover class III-VI disease.
Class III: Focal lupus nephritis
- It accounts for about 9-24% of lupus nephritis biopsies.
- On light microscopy:
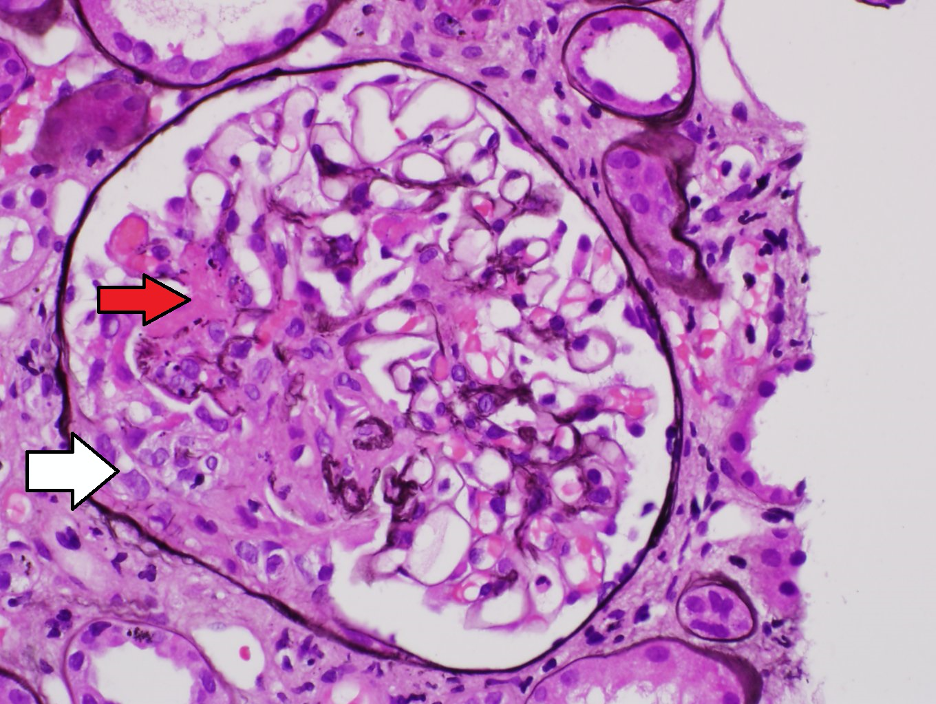
- Focal (less than 50% of total glomeruli) endocapillary hypercellularity characterized by increase of inflammatory cells within capillary loops associated with reactive changes of endothelial cells
- Focal crescentic lesions (defined as 2 or more cells thick associated with involvement of 10% or more of the capsule). Crescentic lesion can be classified into cellular/ fibrocellular crescents and fibrous crescents to evaluate the activity and chronicity of the disease.
- Karyorrhexis, fibrinoid necrosis and associated with disruption of capillary tufts are also noted. (Figure 1)
- Segmental or global glomerulosclerosis may occur in chronic status.
- On immunofluorescence studies:
- Full house staining patterns with coarse granular deposits in segmental distribution along capillary walls chiefly in subendothelial location accompanied by mesangial deposits.
- Scattered subepitheial deposits might be seen.
- Tubulointerstitial and vascular immune deposits might be seen.
- On electron microscopy:
- Segmental electron dense deposits in subendothelial and mesangial areas
- Scattered (less than 50% of glomerular surface area) subepitheial deposits may present
- Deposit in tubular basement membranes can be identified
- Numerous tubuloreticular inclusion bodies can be identified
Note: If the subepithelial deposits are seen in more than 50% of glomerular surface area in at least 50% of the glomeruli, additional diagnosis of membranous lupus nephritis (class V) should be warranted.
Class IV: Diffuse lupus nephritis
- Patients usually have active serologic markers with about 70% have active urinary sediments.
- On light microscopy:
- Active and /or chronic endocapillary and / or extracapillary glomerulonephritis involving more than 50% of the glomeruli
- May show diffuse endocapillary hypercellularity, extensive subendothelial deposits forming a wire-loops lesions, hyaline thrombi, necrotizing lesions and crescents in different combinations
- Mesangial proliferative features are also present.
- Progress to segmental or global glomerulosclerosis might be seen in chronic condition.
- Various degree of acute and chronic tubulointerstitial injury is present and correlated with the severity of acute and chronic glomerular lesion.
- On immunofluorescence studies: Same staining pattern of class III in diffuse fashion.
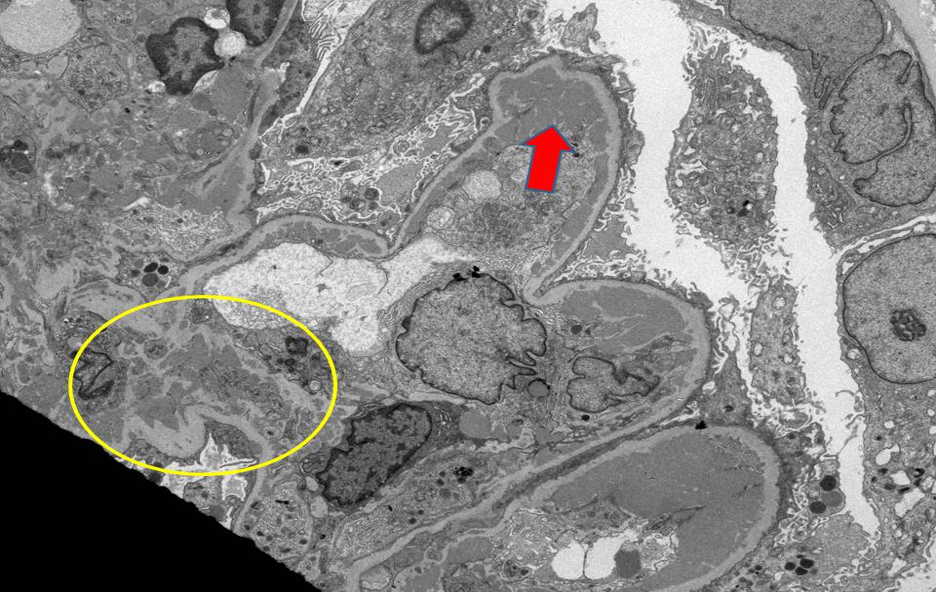
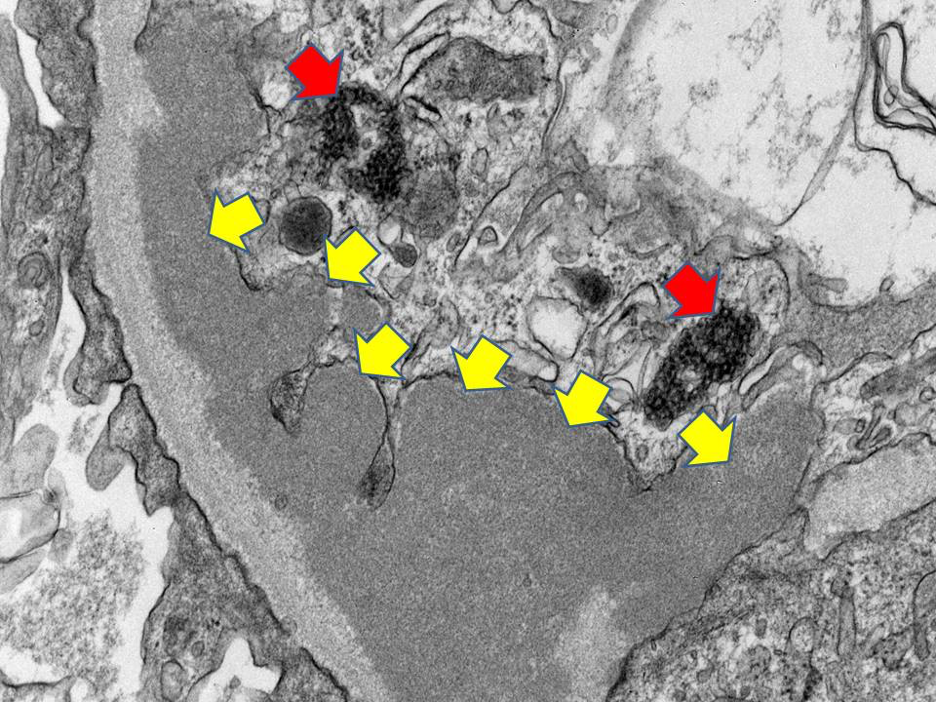
- On electron microscopy: Same findings as class III lupus nephritis in diffuse fashion (Figure 2 and 3)
Note: If the subepithelial deposits are seen in more than 50% of glomerular surface areas in at least 50% of the glomeruli, additional diagnosis of membranous lupus nephritis (class V) should be warranted
Class V: Membranous lupus nephritis
- Patients usually present with heavy proteinuria and nephrotic syndrome
- Hematuria can be seen in half of the patients
- Membranous lupus nephritis could represent an initial clinical presentation without systemic manifestations of lupus
- Patients are at risk for renal vein thrombosis
- On light microscopy:
- In early stages, light microscopic findings may be subtle with slight thickening of glomerular basement membranes
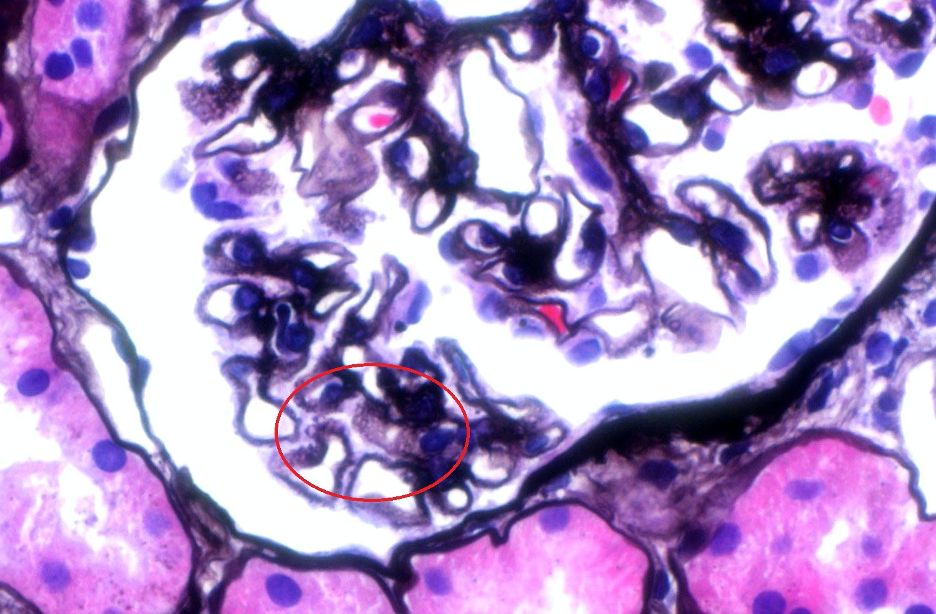
- Later, a full picture of membranous nephropathy is obvious with thickening of capillary wall with spikes and pinholes noted (figure 4)
- Mesangial proliferative features are also present
- In chronic cases, segmental or global glomerulosclerosis might develop
- On immunofluorescence:
- Full house staining patterns with coarse granular deposits in the subepitheial sites with mesangial deposits.
- Occasional small sized subendothelial deposits can been seen
- Extraglomerular deposits can be also seen in the tubular basement membranes and vessels
- On electron microscopy:
- Sizable subepitheial electron-dense deposits along the glomerular basement membranes (figure 5)
- Sparse small subendothelial and paramessangial immune deposits may present.

Class VI: Advanced sclerosing lupus nephritis
- Extensive glomerular scarring with more than 90% global glomerulosclerosis without evidence of residual activity
- This class was introduced to identify cases of aggressive and inactive disease in which aggressive therapy is no long indicated.
Differential diagnosis:
- Type II mixed cryoglobulinemia
- Usually with microtubular substructure type of immune deposits by electron microscopy
- Often associated with hepatitis C virus
- Membranoproliferative glomerulonephritis with immune deposits
- Primary membranous glomerulonephritis
- Absent of extraglomerular deposits
- Absence of subendothelial and mesangial immune-deposits
- Often positive (70%) to phospholipase A2 receptors antibodies
- Lupus-like glomerulonephritis in HIV patients
- Can be found in about 20% of renal biopsies in HIV-infected patients
- Negative to low titer of ANA and DsDNA serologies
- Drug-induced lupus nephritis
- Culprits include hydralazine, isoniazid and procainamide
- Improvement in renal function after drug withdrawal
- Sjogren syndrome
- Often tubulointerstitial nephritis present before the glomerular manifestations
- Positive serologies for Sjogren antibodies
Sam Albadri, MBChB, M.Sc (sam_albadri)
Pathology Fellow, Mayo Clinic
References
Weening JJ et al: J Am Soc Nephrol. 15(2):241-50, 2004
Bajema et al: Kidney Int, 93:789-796, 2018
Austin et al: Kidney Int. 25:689-95, 1984.

