Drug dosage adjustment can be a challenge in patients who develop acute kidney injury (AKI). It is suggested to adopt “a start low and go slow” approach when there is an uncertainty in drug dosing or pharmacokinetics. The important principles that need to be considered include mode of drug elimination, therapeutic target, the initial dose, the maintenance dose, the dose frequency and when the dose adjustment needs to be performed. Nevertheless, therapeutic drug monitoring is one of the tools available (albeit for a handful of drugs), when optimal drug concentrations need to be achieved. Table 1 elucidates markers that indicate clinically significant drug clearance by kidney.
| Table 1. Biochemical and clinical markers of a potentially clinically significant decrease in drug clearance by the kidney (minimum criteria that indicate the potential for impaired kidney function as proposed by Extracorporeal Treatments in Poisoning (EXTRIP) group) |
| eGFR<45 ml/min per 1.73 m2 |
| Stage 2 or 3 AKI |
| In adults without baseline plasma creatinine, plasma creatinine >2 mg/dl (176µmol/L) in adults or 1.5 mg/dl (132µmol/L) in the elderly or those with low muscle mass |
| Plasma creatinine greater than two times the upper limit of normal for age and weight in children without a baseline plasma creatinine concentration |
| The presence of oligo-anuria |
AKI commonly occurs in patients with critical illness . Dosage adjustments are complicated in these patients because of multiple changes that occur in physiology, including organ dysfunction and volume status. The volume of distribution (Vd) often increases in AKI; for example, in critically ill patients with sepsis and AKI, antibiotic Vd varies ten-fold or more. This occurs because of intravenous fluid loading during resuscitation, and capillary leak causing edema, pleural effusions, or ascites, as well as changes in protein binding.
Dose adjustment in AKI is usually based on the present level of kidney function; however estimation of kidney function in AKI is a challenging proposition given the following:
- Individuals have differing metabolic rates.
- Measurements of serum levels always assess kidney function ‘‘in arrears,’’ as they reflect accumulation of the solute in hours and days after the change in eGFR has occurred.
- During an AKI the volume of distribution of these solutes changes rapidly- changes in plasma levels arise not just from alteration in generation and clearance, but also from changes in total body water.
Four-hour creatinine clearance, can give insight into a patient’s kidney function during the interval between administration of a loading dose and the first maintenance dose. The Jelliffe equation was developed to estimate eGFR in AKI, where kidney function is not in steady state. Bouchard and colleagues demonstrated that the Jelliffe equation, modified by consideration of patient volume status, provided a more reliable and accurate assessment of kidney function when compared with timed urine collections in AKI.
There is limited data about the effect of AKI on non-kidney clearance. Changes in bowel, hepatic and kidney perfusion with critical illness may also alter drug absorption and disposition. For some kidney-eliminated drugs, patients with residual renal function will require higher antibiotic doses than their anuric counterparts.
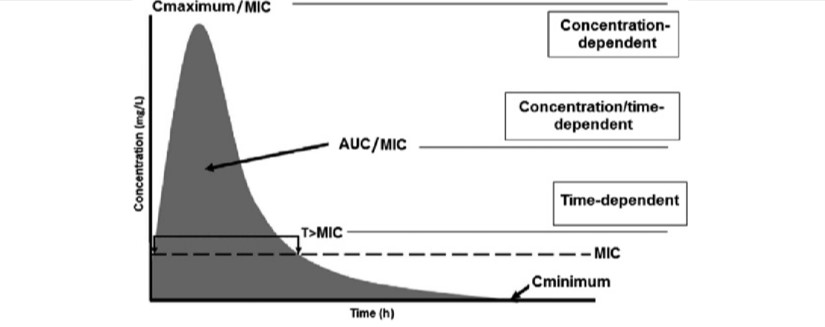
Antibiotics can be thought to exhibit 1 of the 2 different pharmacodynamic profiles; concentration- or time dependent antimicrobial activity. The bacterial killing of time-dependent antibiotics depends on the time the serum concentration is higher than the organism’s minimum inhibitory concentration (MIC). The efficacy of time-dependent antibiotics is enhanced when serum concentration is maintained at 2-4 times the MIC for at least 40% of the dosing interval, although some studies have found best results when time above MIC is 100% of the dosing interval.
Concentration-dependent antibiotics are dependent on reaching high antibiotic serum concentrations. Peak concentration to MIC ratio is used to measure whether pharmacodynamic targets are being met. Antibiotic concentrations targeted are typically 10 or more times the bacterial MIC. In patients managed with intermittent hybrid kidney replacement therapy (KRT), some researchers have suggested that the antibiotic dose should be scheduled before dialysis, so that drug removal by the KRT can be used to avoid toxic effects.
Pharmacodynamic target attainment for the patient receiving KRT in the ICU is a function of the interplay between bacterial sensitivity, drug dosing, pharmacokinetic changes within the critically ill patient, and the KRT selected. Pharmacodynamic target attainment becomes even more difficult when using combination products such as piperacillin/tazobactam, ampicillin/ sulbactam, and trimethoprim/sulfamethoxazole because each component has its own pharmacokinetic properties. Dosing challenges are even greater in patients with AKI receiving KRT when other types of supportive therapy, such as extracorporeal membrane oxygenation or interventional lung assist are required.
What does KDIGO advocate?
Loading dose – As the Vd of many drugs, especially hydrophilic antibiotics (beta-lactams, cephalosporins, and -penems) is significantly increased in the presence of AKI, administration of aggressive loading doses (25–50% greater than normal) is highly recommended.
Maintenance dose – Clinical judgment is paramount and forecasting the degree, rate of change in kidney function and fluid volume status is fraught with uncertainty. Because of the preservation of non-kidney clearance for some agents such as vancomycin, imipenem, and ceftizoxime, as well as the tendency to attain a positive fluid balance in the early stages of AKI, the dosing regimen for many drugs, especially antimicrobial agents, should be initiated at normal or near normal dosage regimens.
Avinash Rao Ullur
Senior Registrar in Nephrology
NU Hospitals, Bengaluru, Karnataka, India
Nice overview.
Other things to consider:
1. what is at stake? Is under treating the infection more worrisome or drug toxicity?
2. Can you measure drug levels?
3. If you have the luxury of having a pharmacist on service, please take their help!
4. Dosing in CRRT & PIRRT is not the same. See some data on pip-taz dosing in SLED: https://pubmed.ncbi.nlm.nih.gov/29730948/ (infusion better than boluses)
Another equation I like to use is the kinetic GFR: https://pubmed.ncbi.nlm.nih.gov/23704286/